

Position Paper for the State-of-the-Art Application of Respiratory Support in Patients with COVID-19
- PMID: 32564028
- PMCID: PMC7360514
- DOI: 10.1159/000509104
Position Paper for the State-of-the-Art Application of Respiratory Support in Patients with COVID-19
Abstract
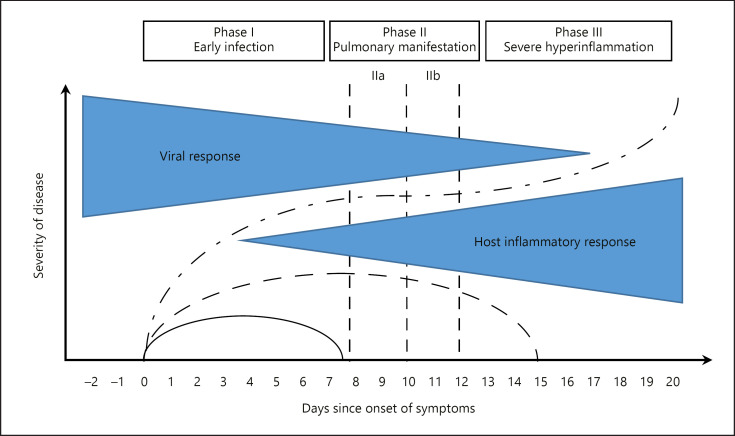
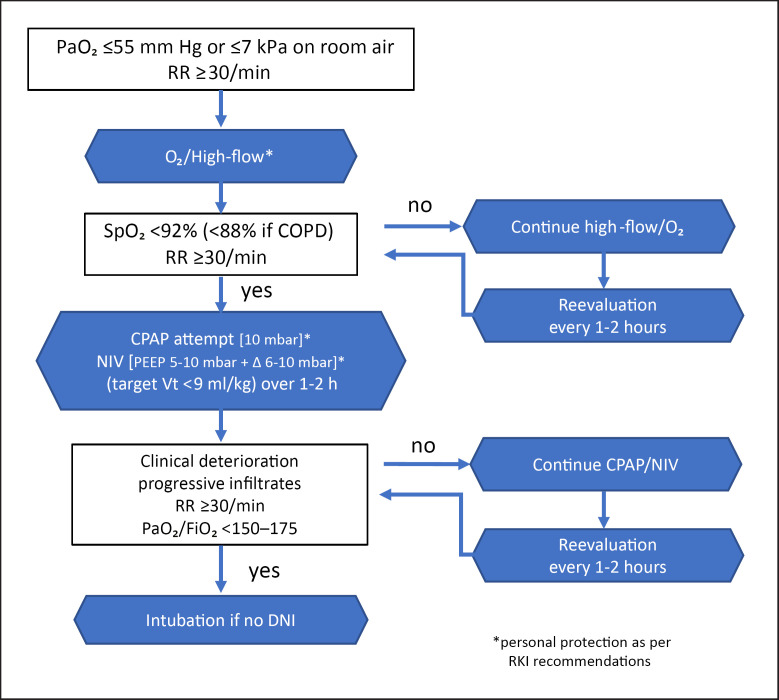
Against the background of the pandemic caused by infection with the SARS-CoV-2 virus, the German Respiratory Society has appointed experts to develop therapy strategies for COVID-19 patients with acute respiratory failure (ARF). Here we present key position statements including observations about the pathophysiology of (ARF). In terms of the pathophysiology of pulmonary infection with SARS-CoV-2, COVID-19 can be divided into 3 phases. Pulmonary damage in advanced COVID-19 often differs from the known changes in acute respiratory distress syndrome (ARDS). Two types (type L and type H) are differentiated, corresponding to early- and late-stage lung damage. This differentiation should be taken into consideration in the respiratory support of ARF. The assessment of the extent of ARF should be based on arterial or capillary blood gas analysis under room air conditions, and it needs to include the calculation of oxygen supply (measured from the variables of oxygen saturation, hemoglobin level, the corrected values of Hüfner's factor, and cardiac output). Aerosols can cause transmission of infectious, virus-laden particles. Open systems or vented systems can increase the release of respirable particles. Procedures in which the invasive ventilation system must be opened and endotracheal intubation carried out are associated with an increased risk of infection. Personal protective equipment (PPE) should have top priority because fear of contagion should not be a primary reason for intubation. Based on the current knowledge, inhalation therapy, nasal high-flow therapy (NHF), continuous positive airway pressure (CPAP), or noninvasive ventilation (NIV) can be performed without an increased risk of infection to staff if PPE is provided. A significant proportion of patients with ARF present with relevant hypoxemia, which often cannot be fully corrected, even with a high inspired oxygen fraction (FiO2) under NHF. In this situation, the oxygen therapy can be escalated to CPAP or NIV when the criteria for endotracheal intubation are not met. In ARF, NIV should be carried out in an intensive care unit or a comparable setting by experienced staff. Under CPAP/NIV, a patient can deteriorate rapidly. For this reason, continuous monitoring and readiness for intubation are to be ensured at all times. If the ARF progresses under CPAP/NIV, intubation should be implemented without delay in patients who do not have a "do not intubate" order.
Keywords: Acute respiratory failure; COVID-19; Respiratory support.
© 2020 S. Karger AG, Basel.
Conflict of interest statement
The authors declare that there are no conflicts of interest.
Figures
References
-
- An der Heiden M, Buchholz U. Modellierung von Beispielszenarien der SARS-CoV-2 Epidemie 2020 in Deutschland [cited 2020] Available from: https://doi. org/10.25646/ 6571.2.
-
- Ewig S, Höffken G, Kern WV, Rohde G, Flick H, Krause R, et al. Behandlung von erwachsenen Patienten mit ambulant erworbener Pneumonie und Prävention - Update 2016. Pneumologie. 2016 Mar;70((3)):151–200. - PubMed
-
- Fichtner F, Moerer O, Laudi S, Weber-Carstens S, Nothacker M, Kaisers U, Investigators and the Guideline Group on Mechanical Ventilation and Extracorporeal Membrane Oxygenation in Acute Respiratory Insufficiency Mechanical Ventilation and Extracorporeal Membrane Oxygenation in Acute Respiratory Insufficiency. Dtsch Arztebl Int. 2018 Dec;115((50)):840–7. - PMC - PubMed
-
- Westhoff M, Schönhofer B, Neumann P, Bickenbach J, Barchfeld T, Becker H, et al. Nicht-invasive Beatmung als Therapie der akuten respiratorischen Insuffizienz. Pneumologie. 2015 Dec;69((12)):719–56. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous