

Risk Factors for Recurrent Staphylococcus aureus Bacteremia
- PMID: 32564065
- PMCID: PMC8315037
- DOI: 10.1093/cid/ciaa801
Risk Factors for Recurrent Staphylococcus aureus Bacteremia
Abstract
Background: To understand the clinical, bacterial, and host characteristics associated with recurrent Staphylococcus aureus bacteremia (R-SAB), patients with R-SAB were compared to contemporaneous patients with a single episode of SAB (S-SAB).
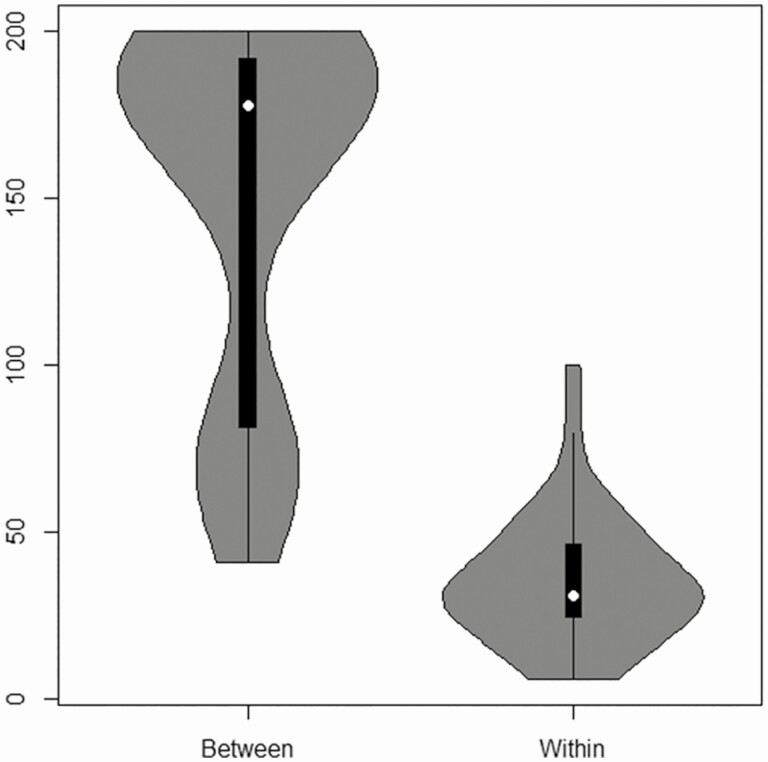
Methods: All SAB isolates underwent spa genotyping. All isolates from R-SAB patients underwent pulsed-field gel electrophoresis (PFGE). PFGE-indistinguishable pairs from 40 patients underwent whole genome sequencing (WGS). Acute phase plasma from R-SAB and S-SAB patients was matched 1:1 for age, race, sex, and bacterial genotype, and underwent cytokine quantification using 25-analyte multiplex bead array.
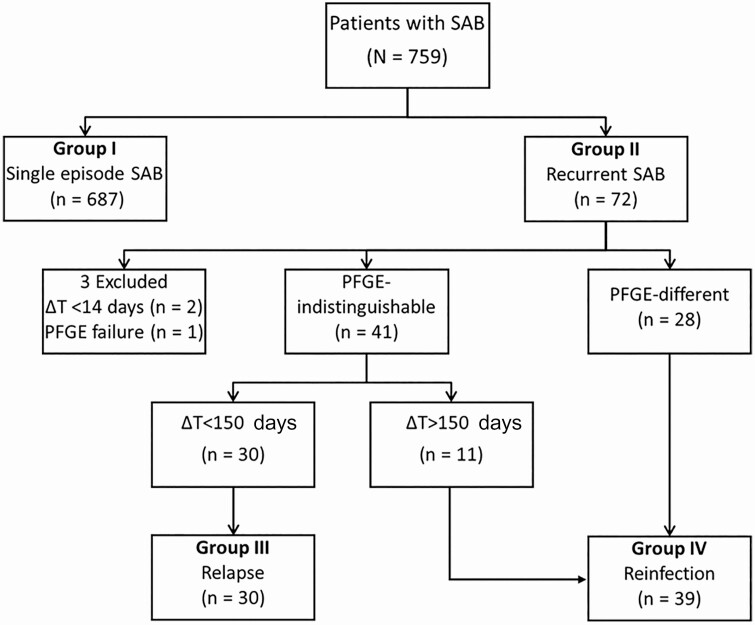
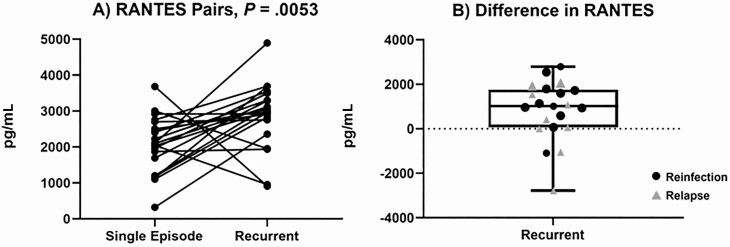
Results: R-SAB occurred in 69 (9.1%) of the 756 study patients. Of the 69 patients, 30 experienced relapse (43.5%) and 39 reinfection (56.5%). Age, race, hemodialysis dependence, presence of foreign body, methicillin-resistant Staphyloccus aureus, and persistent bacteremia were individually associated with likelihood of recurrence. Multivariate risk modeling revealed that black hemodialysis patients were nearly 2 times more likely (odds ratio [OR] = 9.652 [95% confidence interval [CI], 5.402-17.418]) than white hemodialysis patients (OR = 4.53 [95% CI, 1.696-10.879]) to experience R-SAB. WGS confirmed PFGE interpretations in all cases. Median RANTES (regulated on activation, normal T cell expressed and secreted) levels in acute phase plasma from the initial episode of SAB were higher in R-SAB than in matched S-SAB controls (P = .0053, false discovery rate < 0.10).
Conclusion: This study identified several risk factors for R-SAB. The largest risk for R-SAB is among black hemodialysis patients. Higher RANTES levels in R-SAB compared to matched controls warrants further study.
Keywords: Staphylococcus aureus; bacteremia; health disparity; recurrence; whole genome sequencing.
© The Author(s) 2020. Published by Oxford University Press for the Infectious Diseases Society of America. All rights reserved. For permissions, e-mail: journals.permissions@oup.com.
Figures
References
-
- Fowler VGJ, Holland TL. Clinical approach to Staphylococcus aureus bacteremia in adults. In: Lowy FD, ed. UpToDate. Waltham, MA: UpToDate Inc.
-
- Fowler VG Jr, Olsen MK, Corey GR, et al. Clinical identifiers of complicated Staphylococcus aureus bacteremia. Arch Intern Med 2003; 163:2066–72. - PubMed
-
- Hawkins C, Huang J, Jin N, Noskin GA, Zembower TR, Bolon M. Persistent Staphylococcus aureus bacteremia: an analysis of risk factors and outcomes. Arch Intern Med 2007; 167:1861–7. - PubMed
-
- Albertson J, McDanel JS, Carnahan R, et al. Determination of risk factors for recurrent methicillin-resistant Staphylococcus aureus bacteremia in a Veterans Affairs healthcare system population. Infect Control Hosp Epidemiol 2015; 36:543–9. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
