

Pathways to a cancer-free future: a protocol for modelled evaluations to minimise the future burden of colorectal cancer in Australia
- PMID: 32565470
- PMCID: PMC7307542
- DOI: 10.1136/bmjopen-2019-036475
Pathways to a cancer-free future: a protocol for modelled evaluations to minimise the future burden of colorectal cancer in Australia
Abstract
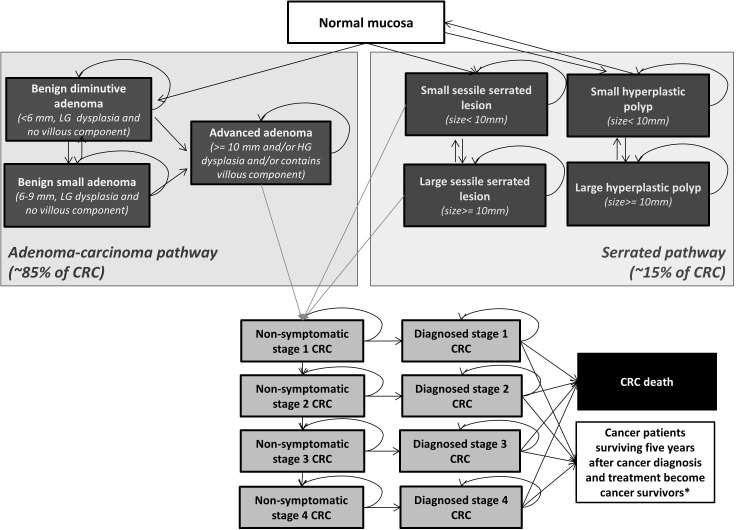
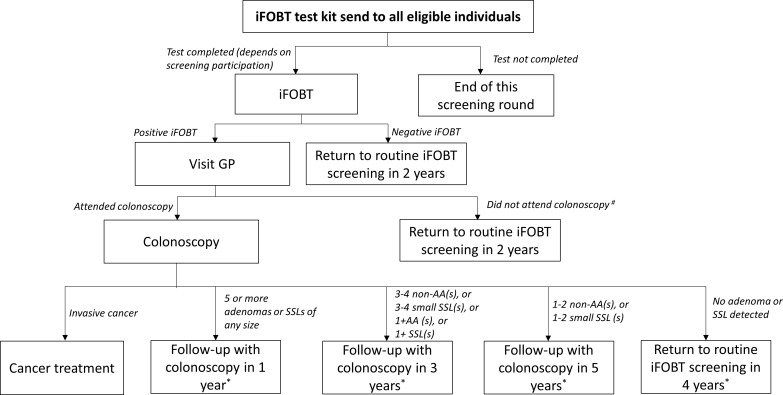
Introduction: With almost 50% of cases preventable and the Australian National Bowel Cancer Screening Program in place, colorectal cancer (CRC) is a prime candidate for investment to reduce the cancer burden. The challenge is determining effective ways to reduce morbidity and mortality and their implementation through policy and practice. Pathways-Bowel is a multistage programme that aims to identify best-value investment in CRC control by integrating expert and end-user engagement; relevant evidence; modelled interventions to guide future investment; and policy-driven implementation of interventions using evidence-based methods. METHODS AND ANALYSIS: Pathways-Bowel is an iterative work programme incorporating a calibrated and validated CRC natural history model for Australia (Policy1-Bowel) and assessing the health and cost outcomes and resource use of targeted interventions. Experts help identify and prioritise modelled evaluations of changing trends and interventions and critically assess results to advise on their real-world applicability. Where appropriate the results are used to support public policy change and make the case for optimal investment in specific CRC control interventions. Fourteen high-priority evaluations have been modelled or planned, including evaluations of CRC outcomes from the changing prevalence of modifiable exposures, including smoking and body fatness; potential benefits of daily aspirin intake as chemoprevention; increasing CRC incidence in people aged <50 years; increasing screening participation in the general and Aboriginal and Torres Strait Islander populations; alternative screening technologies and modalities; and changes to follow-up surveillance protocols. Pathways-Bowel is a unique, comprehensive approach to evaluating CRC control; no prior body of work has assessed the relative benefits of a variety of interventions across CRC development and progression to produce a list of best-value investments.
Ethics and dissemination: Ethics approval was not required as human participants were not involved. Findings are reported in a series of papers in peer-reviewed journals and presented at fora to engage the community and policymakers.
Keywords: colorectal cancer; early detection; prevention; screening.
© Author(s) (or their employer(s)) 2020. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: KC, EF, JW, JBL, EH, MC, NT, KBu and HH receive salary support from CCNSW. KC is co-PI of unrelated investigator-initiated trial of cervical screening in Australia (‘Compass’) conducted by the Victorian Cytology Service, which has received funding contribution from Roche Molecular Systems and Ventana, USA.
Figures
Similar articles
-
The potential for tailored screening to reduce bowel cancer mortality for Aboriginal and Torres Strait Islander peoples in Australia: Modelling study.J Cancer Policy. 2022 Jun;32:100325. doi: 10.1016/j.jcpo.2022.100325. Epub 2022 Feb 8. J Cancer Policy. 2022. PMID: 35560263
-
Australia in 2030: what is our path to health for all?Med J Aust. 2021 May;214 Suppl 8:S5-S40. doi: 10.5694/mja2.51020. Med J Aust. 2021. PMID: 33934362
-
Recalibrating an Established Microsimulation Model to Capture Trends and Projections of Colorectal Cancer Incidence and Mortality.Med Decis Making. 2025 Apr;45(3):257-275. doi: 10.1177/0272989X251314050. Epub 2025 Feb 6. Med Decis Making. 2025. PMID: 39915917
-
A rapid review to inform the policy and practice for the implementation of chronic disease prevention and management programs for Aboriginal and Torres Strait Islander people in primary care.Health Res Policy Syst. 2024 Mar 21;22(1):34. doi: 10.1186/s12961-024-01121-x. Health Res Policy Syst. 2024. PMID: 38509612 Free PMC article.
-
Achieving cultural safety for Australia's First Peoples: a review of the Australian Health Practitioner Regulation Agency-registered health practitioners' Codes of Conduct and Codes of Ethics.Aust Health Rev. 2021 Aug;45(4):398-406. doi: 10.1071/AH20215. Aust Health Rev. 2021. PMID: 33844959 Review.
References
-
- Australian Institute of Health and Welfare Cancer in Australia. Canberra: AIHW, 2019.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical