

Qidong Yixin Oral Liquid for Viral Myocarditis: A Systematic Review and Meta-Analysis
- PMID: 32565861
- PMCID: PMC7261334
- DOI: 10.1155/2020/4704535
Qidong Yixin Oral Liquid for Viral Myocarditis: A Systematic Review and Meta-Analysis
Abstract
Objective: This study aimed to evaluate the efficacy and safety of Qidong Yixin (QY) oral liquid in the treatment of viral myocarditis (VMC).
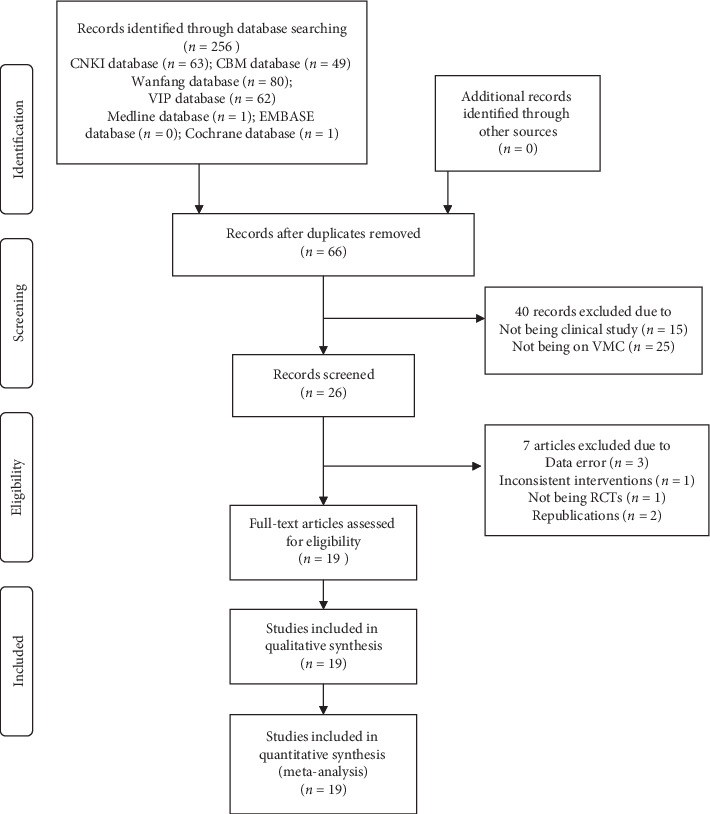
Methods: We searched seven databases for randomized clinical trials on QY for treating VMC. The retrieval period was from database establishment to December 31, 2019. Cochrane risk of bias tool in the Cochrane Handbook was used to assess the methodological quality. Review Manager (RevMan) 5.3 was used to analyze the results.
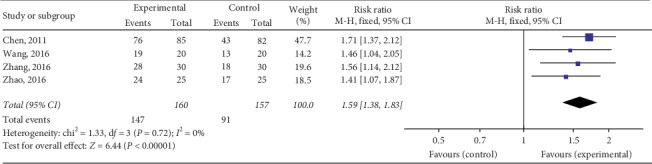
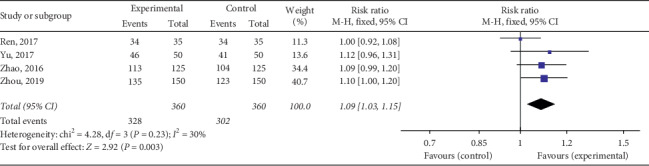
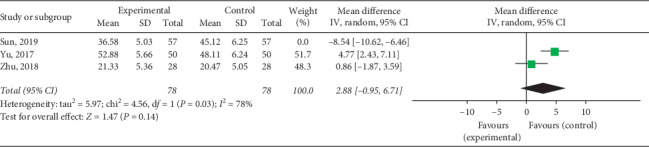
Results: We included 19 studies comprising 2,608 patients, albeit with low methodological quality. Our meta-analysis revealed that combination therapy with QY and western medicine was more effective than western medicine alone (QY vs other Chinese patent medicines: RR = 1.37, 95% Cl: 1.23∼1.52, P < 0.00001; QY + coenzyme Q10 + routine treatment vs coenzyme Q10 + routine treatment: RR = 1.20, 95% Cl: 1.14∼1.27, P < 0.00001; QY + trimetazidine + acyclovir vs trimetazidine + acyclovir: RR = 1.59, 95% Cl: 1.38∼1.83, P < 0.00001; QY + routine treatment vs routine treatment: RR = 1.09, 95% Cl: 1.03∼1.15, P < 0.003). A study on posttreatment myocardial enzyme levels revealed that QY with western medicine downregulated creatine kinase isoenzyme (CK-MB) (QY + antiviral treatment + routine treatment vs antiviral treatment + routine treatment group: MD = -11.28, 95% CI: -13.33∼-9.22, P < 0.00001; QY + routine treatment vs routine treatment: MD = -4.96, 95% CI: -5.56∼-4.32, P < 0.00001), creatine kinase (CK) (MD = -32.10, 95% CI: -35.63∼-28.57, P < 0.00001), and lactate dehydrogenase (LDH) (QY + antiviral treatment + routine treatment vs antiviral treatment + routine treatment: MD = -48.76 95% CI: -58.18∼-39.33, P < 0.00001; QY + routine treatment vs routine treatment: MD = -23.52, 95% CI: -30.10-16.94, P < 0.00001) rather than western medicine alone, with no evidence of aspartate aminotransferase (AST) downregulation on treatment with QY with western medicine (MD = 2.88, 95% CI: -0.95∼6.71, P < 0.00001) in patients. Two studies reported adverse events, indicating that QY is relatively safe.
Conclusion: Although QY may have potential advantages in treating VMC, they remain unclear owing to the poor methodological quality of most studies. Larger, multicenter, high-quality randomized controlled trials are required to verify the effectiveness of QY.
Copyright © 2020 Jun Hu et al.
Conflict of interest statement
All authors declare no conflicts of interest.
Figures










Similar articles
-
Effectiveness and Safety of Shengmai San for Viral Myocarditis: A Systematic Review and Meta-Analysis of Randomized Controlled Trials.Cardiovasc Ther. 2024 Jun 20;2024:2127018. doi: 10.1155/2024/2127018. eCollection 2024. Cardiovasc Ther. 2024. PMID: 39742019 Free PMC article.
-
[Systematic review and Meta-analysis on efficacy and safety of Naoxueshu Oral Liquid in treatment of hypertensive intracerebral hemorrhage].Zhongguo Zhong Yao Za Zhi. 2021 Jun;46(12):2984-2994. doi: 10.19540/j.cnki.cjcmm.20210324.501. Zhongguo Zhong Yao Za Zhi. 2021. PMID: 34467688 Chinese.
-
The Effectiveness and Safety of Moxibustion for Treating Knee Osteoarthritis: A PRISMA Compliant Systematic Review and Meta-Analysis of Randomized Controlled Trials.Pain Res Manag. 2019 Dec 17;2019:2653792. doi: 10.1155/2019/2653792. eCollection 2019. Pain Res Manag. 2019. PMID: 31949547 Free PMC article.
-
Evaluation of the Efficacy and Safety of Chinese Herbal Injection Combined With Trimetazidine for Viral Myocarditis: A Network Meta-Analysis.Front Pharmacol. 2021 Apr 29;12:630896. doi: 10.3389/fphar.2021.630896. eCollection 2021. Front Pharmacol. 2021. PMID: 33995029 Free PMC article. Review.
-
[Pharmacoeconomic evaluation of Qidong Yixin Oral Liquid in treatment of viral myocarditis (Qi-Yin deficiency syndrome) with TreeAge Pro].Zhongguo Zhong Yao Za Zhi. 2022 Feb;47(3):829-835. doi: 10.19540/j.cnki.cjcmm.20211115.501. Zhongguo Zhong Yao Za Zhi. 2022. PMID: 35178966 Chinese.
References
-
- Caforio A. L. P., Pankuweit S., Arbustini E., et al. Current state of knowledge on aetiology, diagnosis, management, and therapy of myocarditis: a position statement of the European Society of Cardiology Working Group on Myocardial and Pericardial Diseases. European Heart Journal. 2013;34(33):2636–2648. doi: 10.1093/eurheartj/eht210. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
