

Application of immune checkpoint inhibitors in EGFR-mutant non-small-cell lung cancer: from bed to bench
- PMID: 32565926
- PMCID: PMC7285948
- DOI: 10.1177/1758835920930333
Application of immune checkpoint inhibitors in EGFR-mutant non-small-cell lung cancer: from bed to bench
Abstract
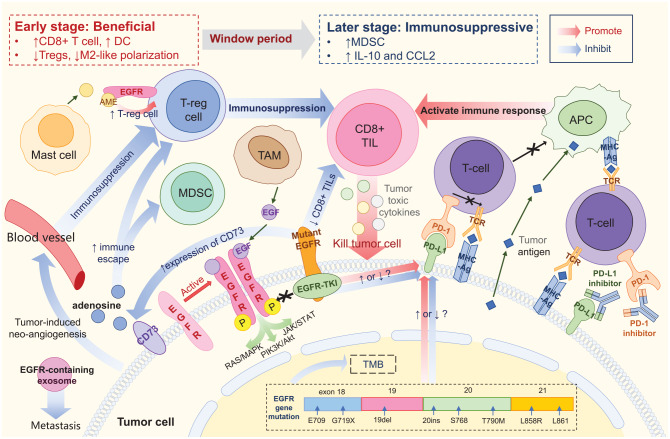
Targeted therapies are efficient in the context of oncogenic driver mutations. Epidermal growth factor receptor (EGFR)-mutant lung cancers represent a distinct subset of non-small-cell lung cancer (NSCLC) with marked sensitivity to EGFR tyrosine kinase inhibitors (TKIs). Despite the high response rate to EGFR TKIs in EGFR-mutant lung cancer, resistance and tumor recurrence are unavoidable. Therapeutic options are restricted in patients after exhaustion of targeted therapies. Immune checkpoint inhibitors (ICIs) represent a novel therapeutic option for advanced NSCLC with significant overall survival benefit in registration trials. No superiority in terms of long-term survival was observed in the EGFR mutation subgroup when ICIs were given as monotherapy in second-line treatment in earlier studies. Thus, the appropriate application of ICIs to patients harboring EGFR mutations remains an important field of ongoing research. Here, we discuss different immune checkpoint blockade strategies, including ICIs alone and in combination with TKIs, chemotherapy, radiation, and antiangiogenic agents in EGFR-mutant NSCLC as first-line and subsequent treatments. We also summarize the evidence concerning the heterogeneous molecular features and immune signatures of EGFR mutations and their associations with ICI therapy outcomes. This study was performed to improve our understanding of the optimal mode of immune-based treatment approaches in EGFR-mutant NSCLC.
Keywords: epidermal growth factor receptor; immune checkpoint inhibitor; non-small-cell lung cancer; tumor microenvironment.
© The Author(s), 2020.
Conflict of interest statement
Conflict of interest: The authors declare that there is no conflict of interest.
Figures
References
-
- Fukuoka M, Wu YL, Thongprasert S, et al. Biomarker analyses and final overall survival results from a phase III, randomized, open-label, first-line study of gefitinib versus carboplatin/paclitaxel in clinically selected patients with advanced non-small-cell lung cancer in Asia (IPASS). J Clin Oncol 2011; 29: 2866–2874. - PubMed
-
- Soria JC, Ohe Y, Vansteenkiste J, et al. Osimertinib in untreated EGFR-mutated advanced non-small-cell lung cancer. N Engl J Med 2018; 378: 113–125. - PubMed
-
- Reck M, Rodriguez-Abreu D, Robinson AG, et al. Pembrolizumab versus chemotherapy for PD-L1-positive non-small-cell lung cancer. N Engl J Med 2016; 375: 1823–1833. - PubMed
-
- Socinski MA, Jotte RM, Cappuzzo F, et al. Atezolizumab for first-line treatment of metastatic nonsquamous NSCLC. N Engl J Med 2018; 378: 2288–2301. - PubMed
-
- Gandhi L, Rodriguez-Abreu D, Gadgeel S, et al. Pembrolizumab plus chemotherapy in metastatic non-small-cell lung cancer. N Engl J Med 2018; 378: 2078–2092. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
