

Predicting Liver Disease Risk Using a Combination of Common Clinical Markers: A Screening Model from Routine Health Check-Up
- PMID: 32566041
- PMCID: PMC7281844
- DOI: 10.1155/2020/8460883
Predicting Liver Disease Risk Using a Combination of Common Clinical Markers: A Screening Model from Routine Health Check-Up
Abstract
Background: Early detection is crucial for the prognosis of patients with autoimmune liver disease (AILD). Due to the relatively low incidence, developing screening tools for AILD remain a challenge.
Aims: To analyze clinical characteristics of AILD patients at initial presentation and identify clinical markers, which could be useful for disease screening and early detection.
Methods: We performed observational retrospective study and analyzed 581 AILD patients who were hospitalized in the gastroenterology department and 1000 healthy controls who were collected from health management center. Baseline characteristics at initial presentation were used to build regression models. The model was validated on an independent cohort of 56 patients with AILD and 100 patients with other liver disorders.
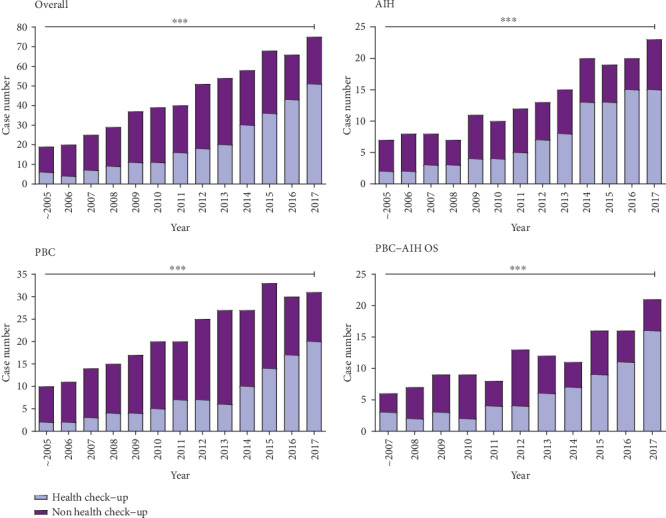
Results: Asymptomatic AILD individuals identified by the health check-up are increased yearly (from 31.6% to 68.0%, p < 0.001). The cirrhotic rates at an initial presentation are decreased in the past 18 years (from 52.6% to 20.0%, p < 0.001). Eight indicators, which are common in the health check-up, are independent risk factors of AILD. Among them, abdominal lymph node enlargement (LN) positive is the most significant different (OR 8.85, 95% CI 2.73-28.69, p < 0.001). The combination of these indicators shows high predictive power (AUC = 0.98, sensitivity 89.0% and specificity 96.4%) for disease screening. Except two liver or cholangetic injury makers, the combination of AGE, GENDER, GLB, LN, concomitant extrahepatic autoimmune diseases, and familial history also shows a high predictive power for AILD in other liver disorders (AUC = 0.91).
Conclusion: Screening for AILD with described parameters can detect AILD in routine health check-up early, effectively and economically. Eight variables in routine health check-up are associated with AILD and the combination of them shows good ability of identifying high-risk individuals.
Copyright © 2020 Yi Wang et al.
Conflict of interest statement
The authors declare no conflict of interest.
Figures




References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
