

The role of viral co-infections in the severity of acute respiratory infections among children infected with respiratory syncytial virus (RSV): A systematic review and meta-analysis
- PMID: 32566164
- PMCID: PMC7295447
- DOI: 10.7189/jogh.10.010426
The role of viral co-infections in the severity of acute respiratory infections among children infected with respiratory syncytial virus (RSV): A systematic review and meta-analysis
Abstract
Background: Respiratory syncytial virus (RSV) is the predominant viral cause of childhood pneumonia. Little is known about the role of viral-coinfections in the clinical severity in children infected with RSV.
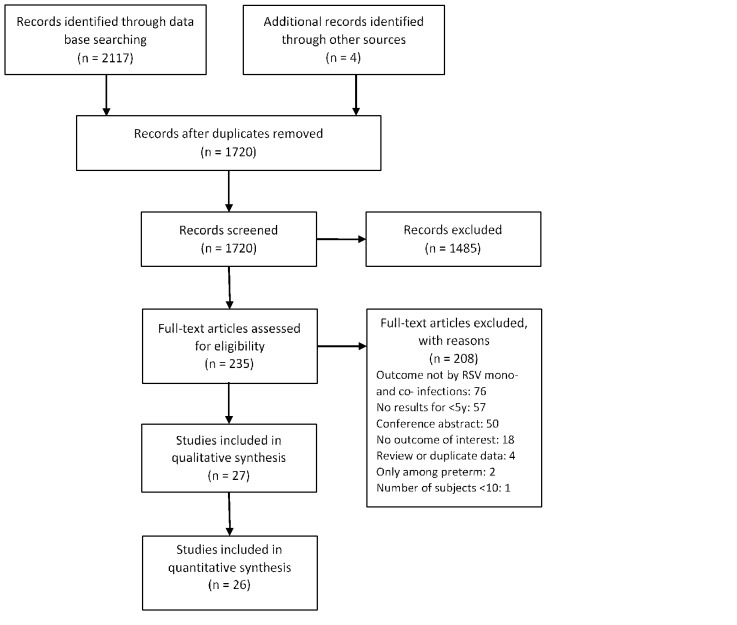
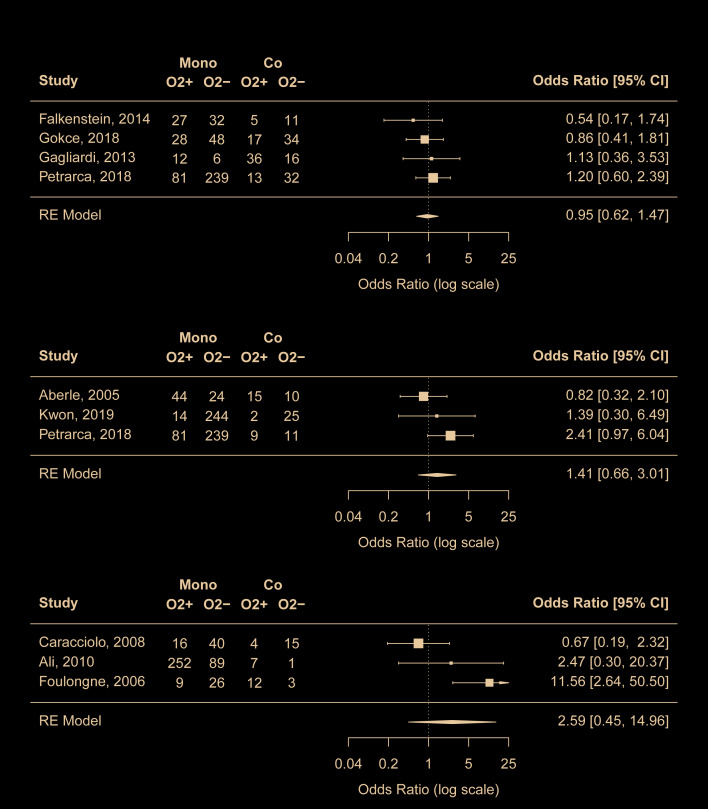
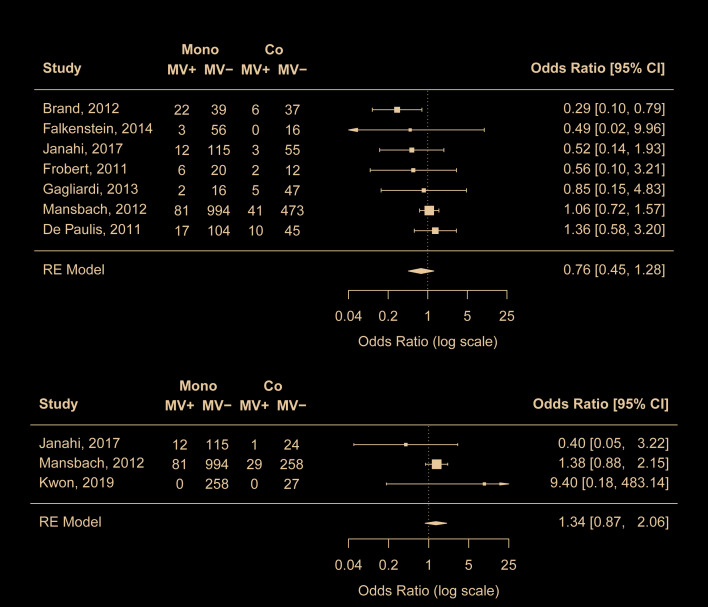
Methods: We conducted a systematic literature review of publications comparing the clinical severity between RSV mono-infection and RSV co-infection with other viruses in children under five years (<5y). Clinical severity was measured using the following six clinical outcomes: hospitalisation, length of hospital stay, use of supplemental oxygen, intensive care unit (ICU) admission, mechanical ventilation and deaths. We summarised the findings by clinical outcome and conducted random-effect meta-analyses, where applicable, to quantitatively synthesize the association between RSV mono-infection/RSV co-infection and the clinical severity.
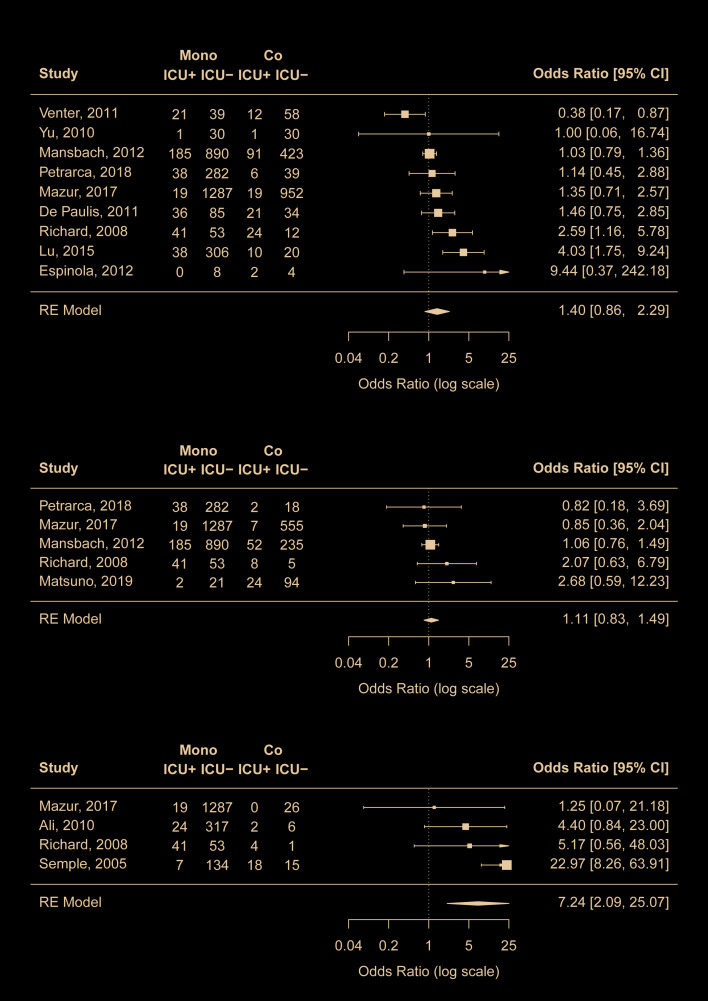
Results: Overall, no differences in the clinical severity were found between RSV mono-infection and RSV co-infection with any viruses, except for the RSV-human metapneumovirus (hMPV) co-infection. RSV-hMPV coinfection was found to be associated with a higher risk of ICU admission (odds ratio (OR) = 7.2, 95% confidence interval (CI) = 2.1-25.1; OR after removal of the most influential study was 3.7, 95% CI = 1.1-12.3). We also observed a trend from three studies that RSV-hMPV coinfections were likely to be associated with longer hospital stay.
Conclusion: Our findings suggest that RSV-hMPV coinfections might be associated with increased risk for ICU admission in children <5y compared with RSV mono-infection but such association does not imply causation. Our findings do not support the association between RSV coinfections with other viruses and clinical severity but further large-scale investigations are needed to confirm the findings.
Protocol registration: PROSPERO CRD42019154761.
Copyright © 2020 by the Journal of Global Health. All rights reserved.
Conflict of interest statement
Competing interests: YL, PP and FM have no competing interests to declare. HN reports grants and personal fees from Innovative Medicines Initiative, grants from World Health Organization, personal fees from Bill and Melinda Gates Foundation, grants and personal fees from Sanofi, personal fees from Janssen, personal fees from AbbVie, grants from National Institute of Health Research, outside the submitted work. The authors have completed the ICMJE conflict of interest form (available upon request from the corresponding author), and declare no further conflicts of interest.
Figures
References
-
- Shi T, McAllister DA, O’Brien KL, Simoes EAF, Madhi SA, Gessner BD, et al. Global, regional, and national disease burden estimates of acute lower respiratory infections due to respiratory syncytial virus in young children in 2015: a systematic review and modelling study. Lancet. 2017;390:946-58. 10.1016/S0140-6736(17)30938-8 - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
