

An organosynthetic soft robotic respiratory simulator
- PMID: 32566890
- PMCID: PMC7286700
- DOI: 10.1063/1.5140760
An organosynthetic soft robotic respiratory simulator
Abstract
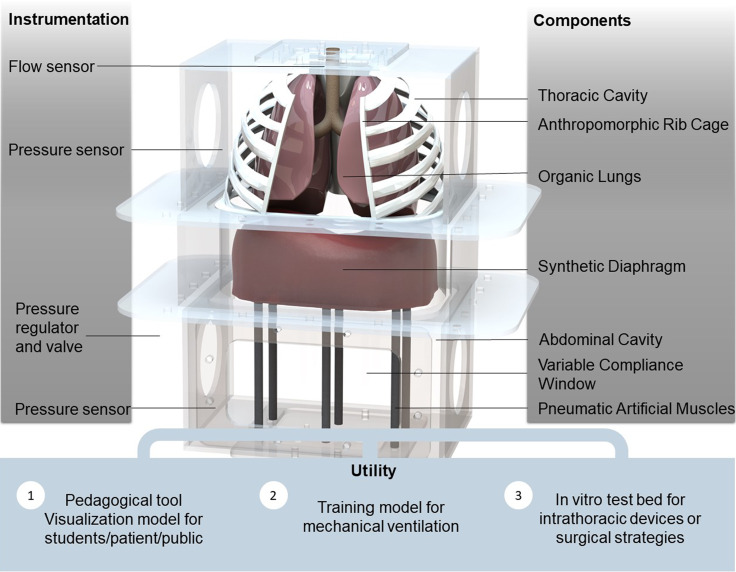
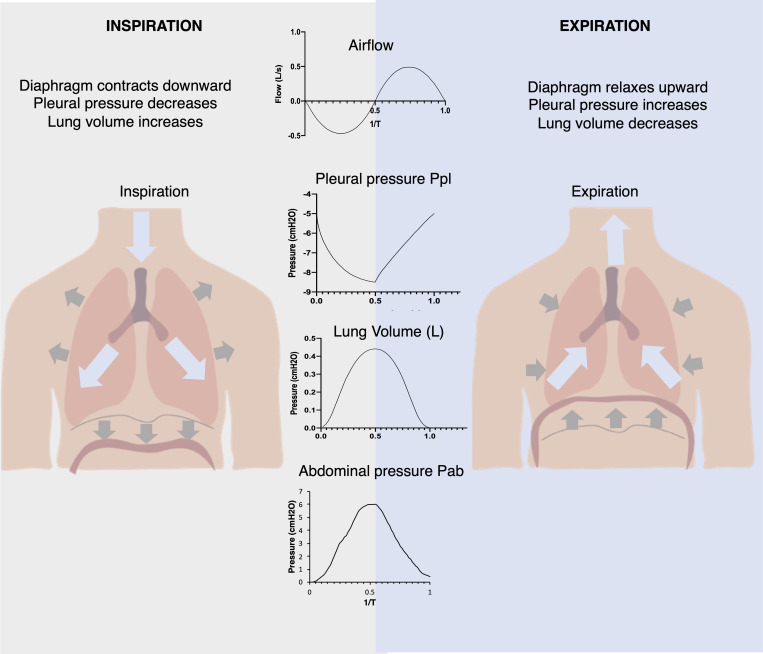
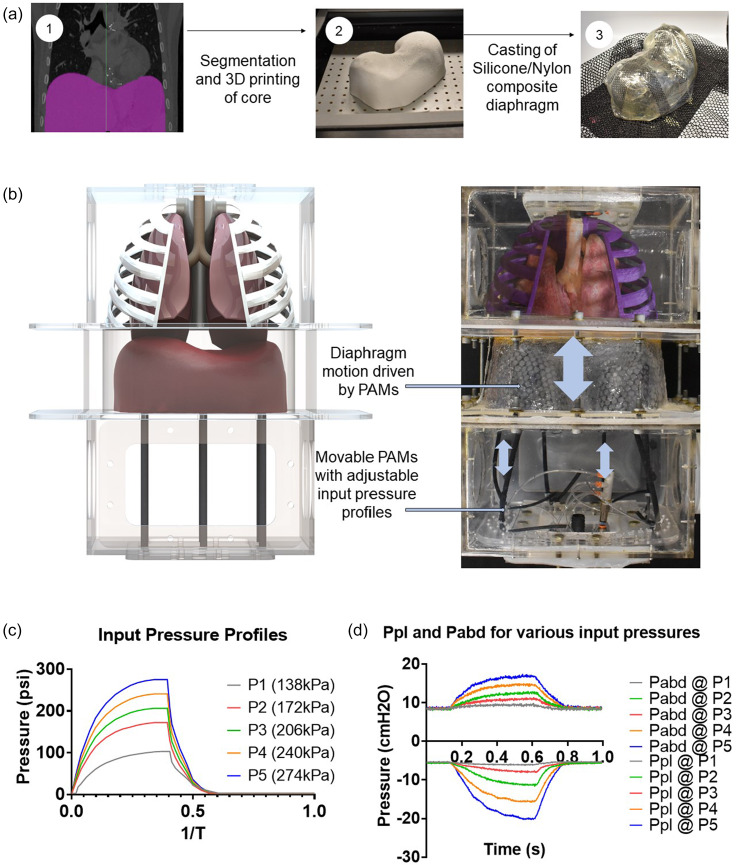
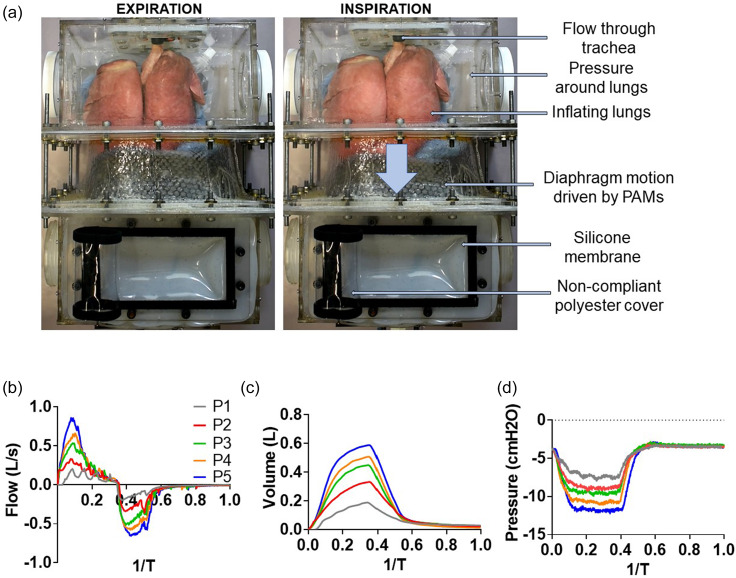
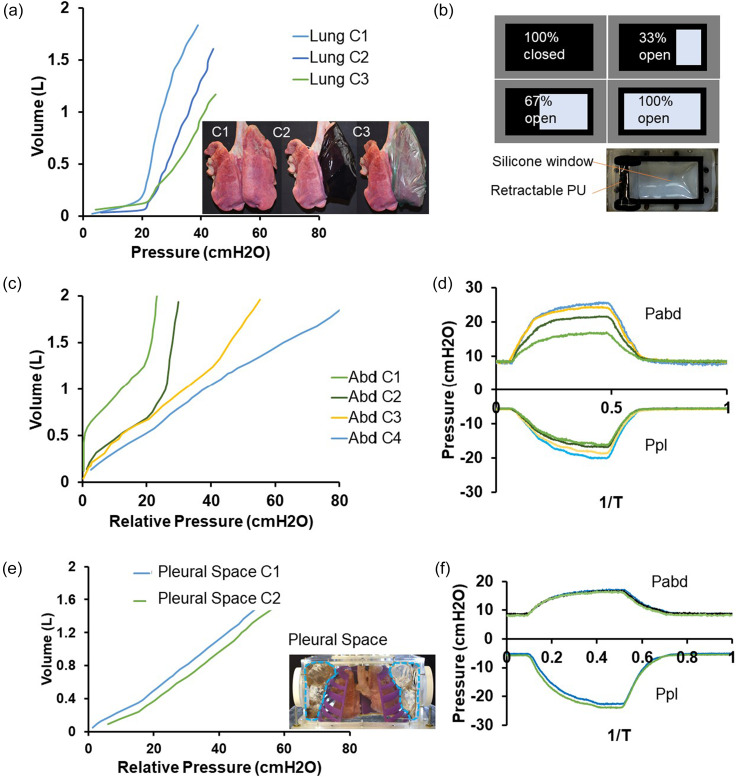
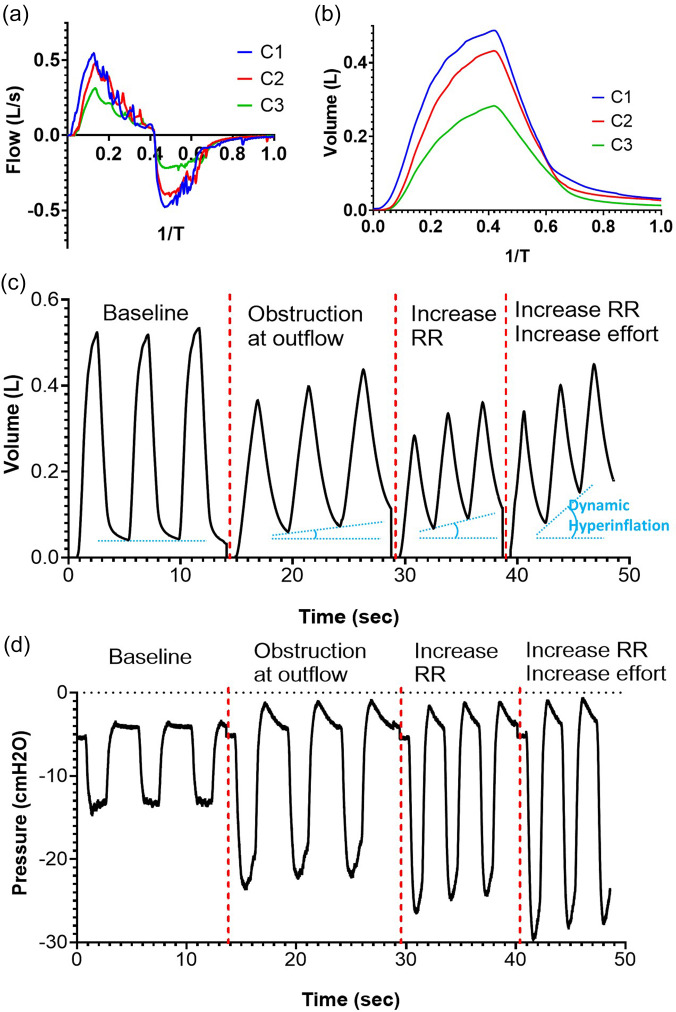
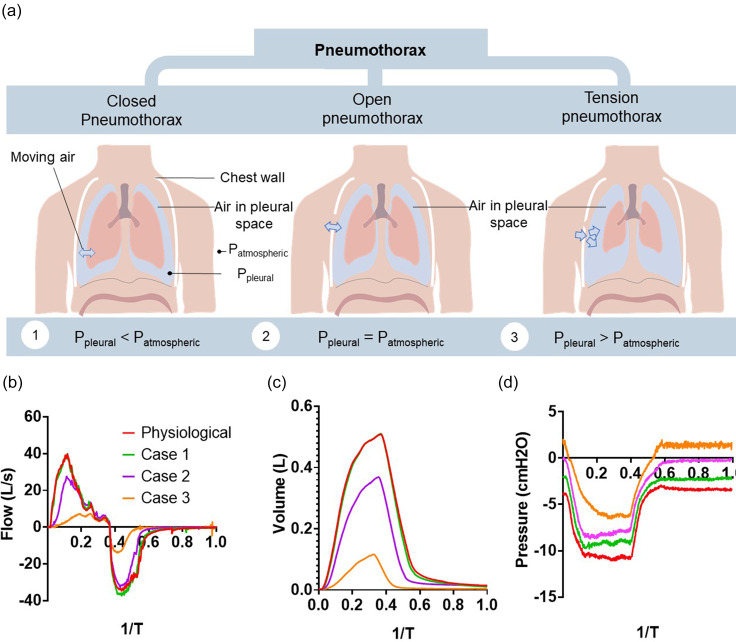
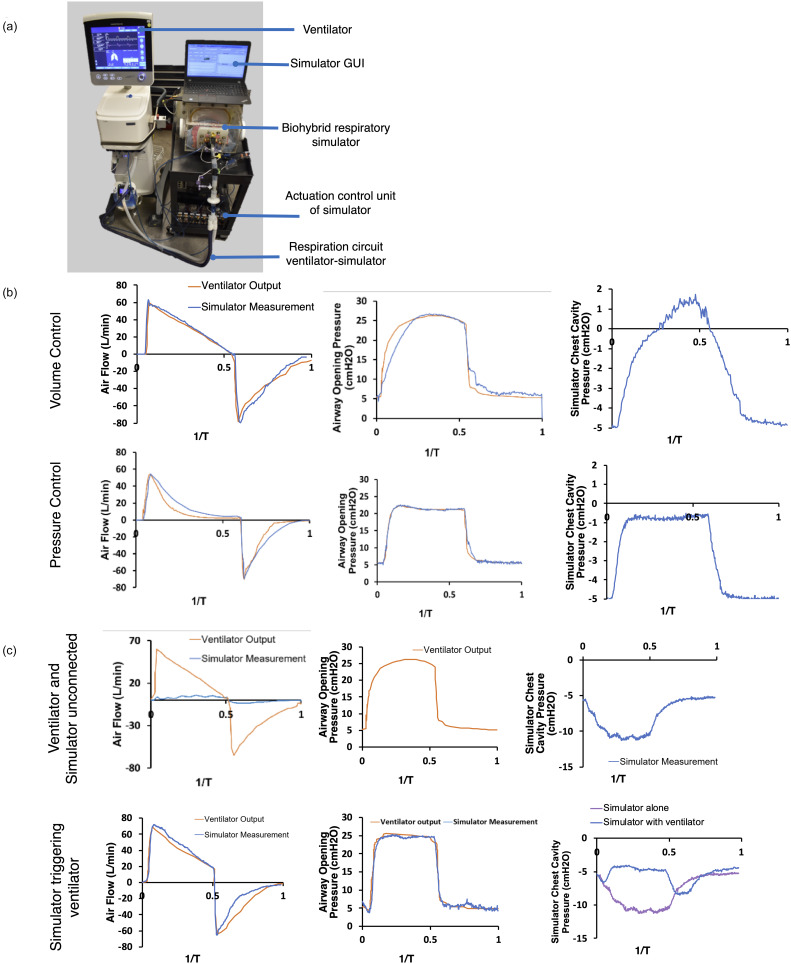
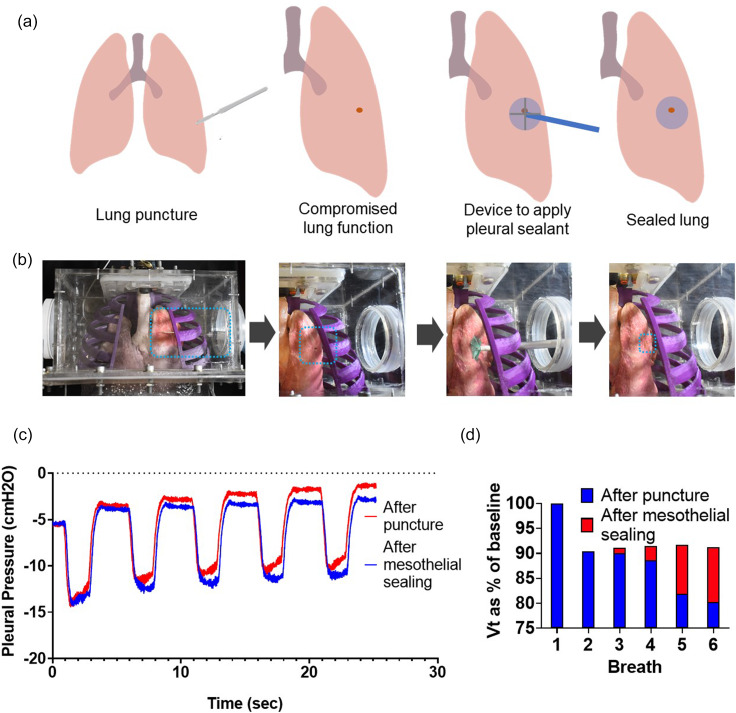
In this work, we describe a benchtop model that recreates the motion and function of the diaphragm using a combination of advanced robotic and organic tissue. First, we build a high-fidelity anthropomorphic model of the diaphragm using thermoplastic and elastomeric material based on clinical imaging data. We then attach pneumatic artificial muscles to this elastomeric diaphragm, pre-programmed to move in a clinically relevant manner when pressurized. By inserting this diaphragm as the divider between two chambers in a benchtop model-one representing the thorax and the other the abdomen-and subsequently activating the diaphragm, we can recreate the pressure changes that cause lungs to inflate and deflate during regular breathing. Insertion of organic lungs in the thoracic cavity demonstrates this inflation and deflation in response to the pressures generated by our robotic diaphragm. By tailoring the input pressures and timing, we can represent different breathing motions and disease states. We instrument the model with multiple sensors to measure pressures, volumes, and flows and display these data in real-time, allowing the user to vary inputs such as the breathing rate and compliance of various components, and so they can observe and measure the downstream effect of changing these parameters. In this way, the model elucidates fundamental physiological concepts and can demonstrate pathology and the interplay of components of the respiratory system. This model will serve as an innovative and effective pedagogical tool for educating students on respiratory physiology and pathology in a user-controlled, interactive manner. It will also serve as an anatomically and physiologically accurate testbed for devices or pleural sealants that reside in the thoracic cavity, representing a vast improvement over existing models and ultimately reducing the requirement for testing these technologies in animal models. Finally, it will act as an impactful visualization tool for educating and engaging the broader community.
© 2020 Author(s).
Figures
References
-
- Yip D. Y., “ An improved model for demonstrating the mechanism of breathing,” Am. Biol. Teach. 60, 528–530 (1998).10.2307/4450538 - DOI
LinkOut - more resources
Full Text Sources
Other Literature Sources