

Complement activation profile of patients with primary focal segmental glomerulosclerosis
- PMID: 32569286
- PMCID: PMC7307932
- DOI: 10.1371/journal.pone.0234934
Complement activation profile of patients with primary focal segmental glomerulosclerosis
Abstract
Background: Studies on adriamycin mice model suggest complement system is activated and together with IgM contributes to the glomerular injury of primary focal segmental glomerulosclerosis (FSGS). We recently reported primary FSGS patients with IgM and C3 deposition showed unfavorable therapeutic responses and worse renal outcomes. Here we examined the plasma and urinary complement profile of patients with primary FSGS, aiming to investigate the complement participation in FSGS pathogenesis.
Methods: Seventy patients with biopsy-proven primary FSGS were enrolled. The plasma and urinary levels of C3a, C5a, soluble C5b-9, C4d, C1q, MBL, and Bb were determined by commercial ELISA kits.
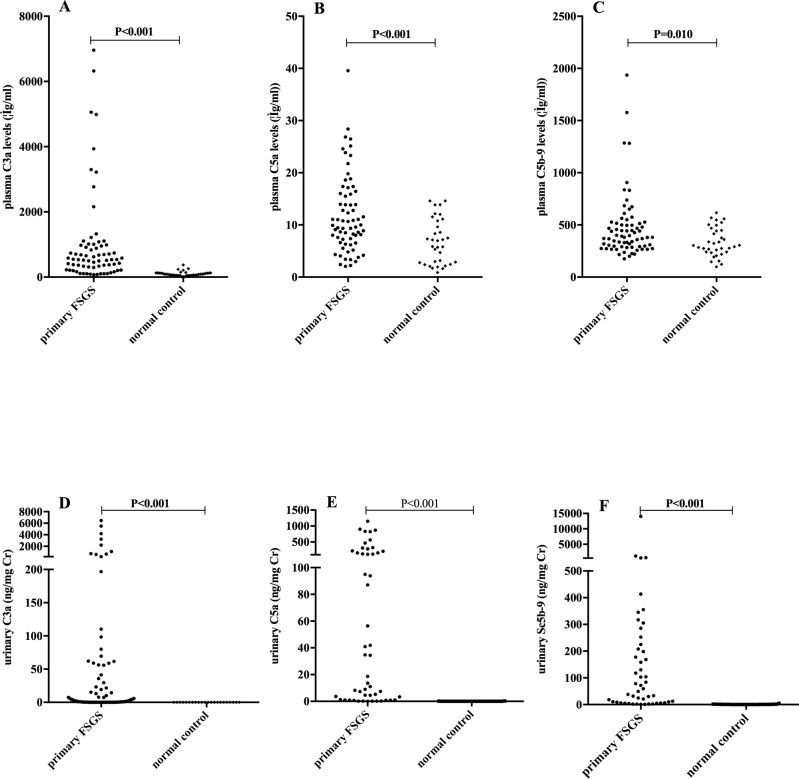
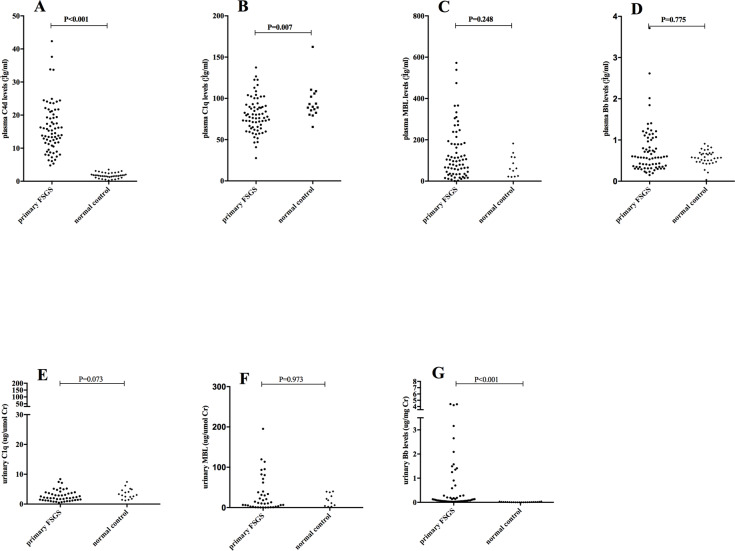
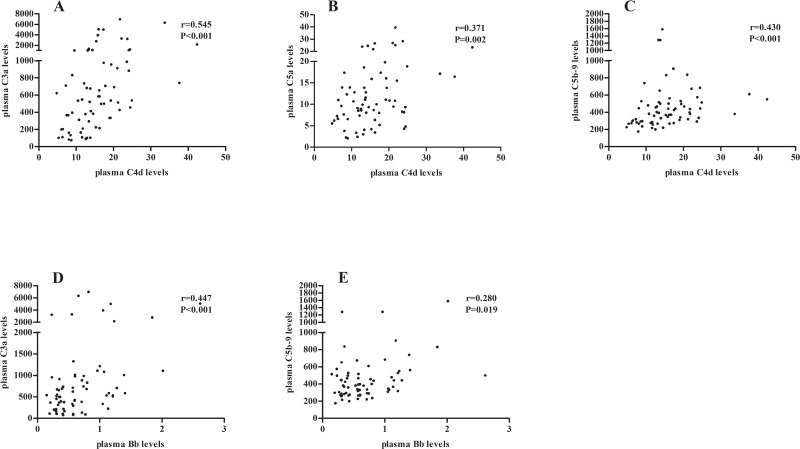
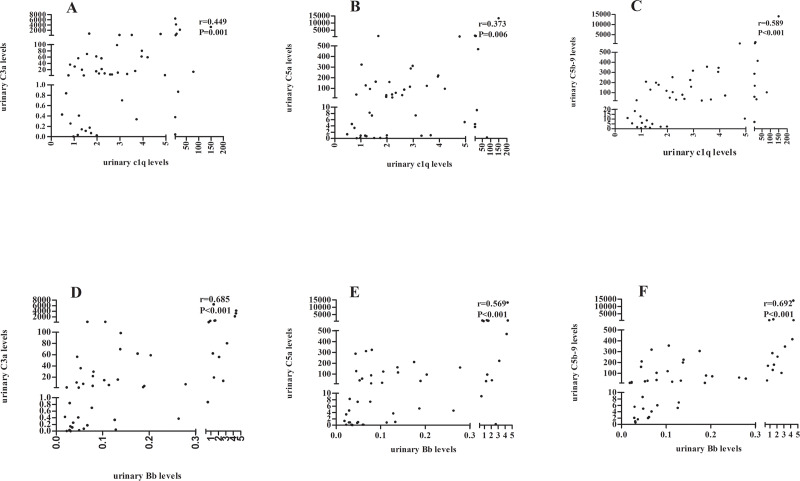
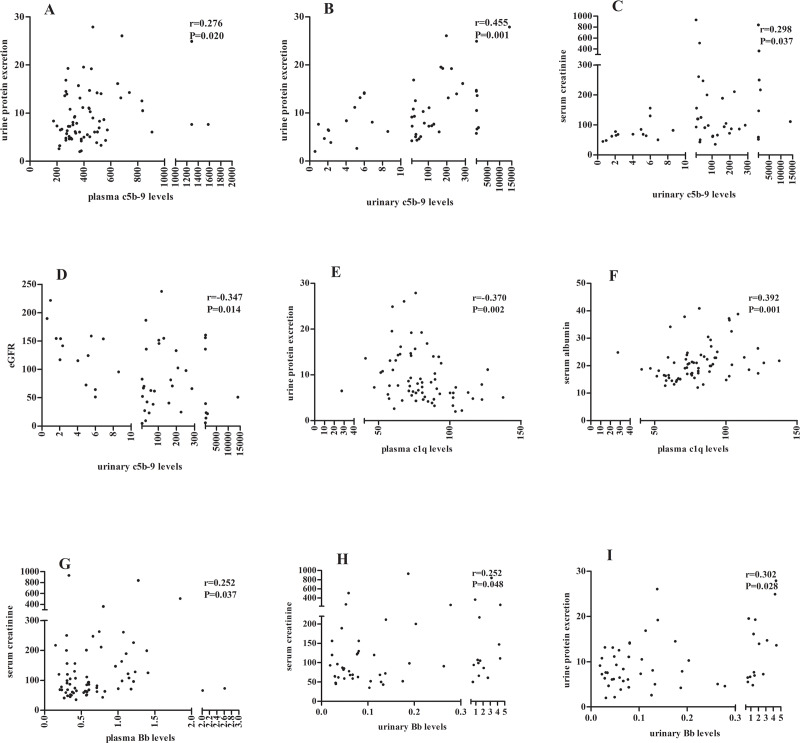
Results: The levels of C3a, C5a and C5b-9 in plasma and urine of FSGS patients were significantly higher than those in normal controls. The plasma and urinary levels of C5b-9 were positively correlated with urinary protein, renal dysfunction and interstitial fibrosis. The plasma C5a levels were positively correlated with the proportion of segmental sclerotic glomeruli. The urinary levels of Bb were elevated, positively correlated with C3a and C5b-9 levels, renal dysfunction, and interstitial fibrosis. The plasma C1q level was significantly decreased, and negatively correlated with urinary protein excretion. Urinary Bb level was a risk factor for no remission (HR = 3.348, 95% CI 1.264-8.870, P = 0.015) and ESRD (HR = 2.323, 95% CI 1.222-4.418, P = 0.010).
Conclusion: In conclusion, our results identified the systemic activation of complement in human primary FSGS, possibly via the classical and alternative pathway. The activation of complement system was partly associated with the clinical manifestations, kidney pathological damage, and renal outcomes.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
