

Recombinant Acid Ceramidase Reduces Inflammation and Infection in Cystic Fibrosis
- PMID: 32569477
- PMCID: PMC7560813
- DOI: 10.1164/rccm.202001-0180OC
Recombinant Acid Ceramidase Reduces Inflammation and Infection in Cystic Fibrosis
Abstract
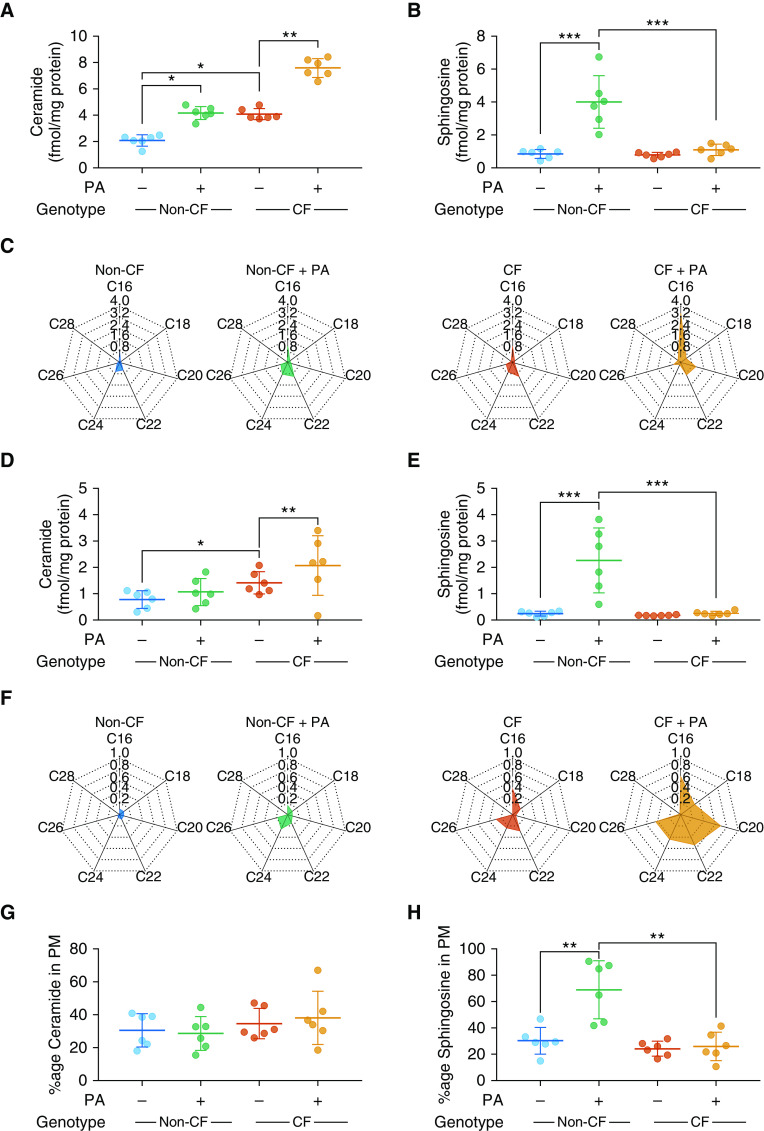
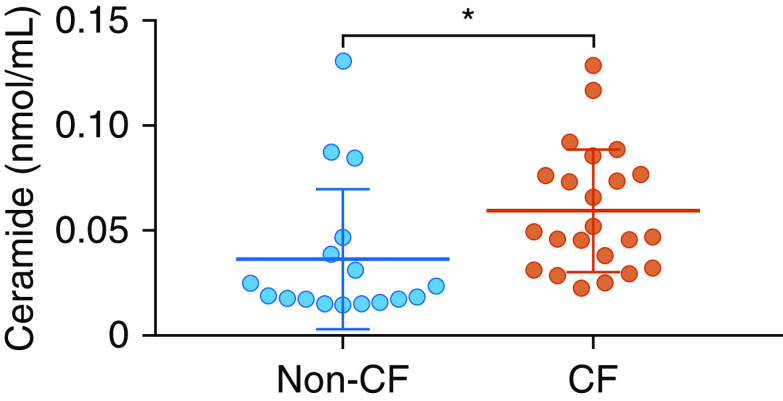
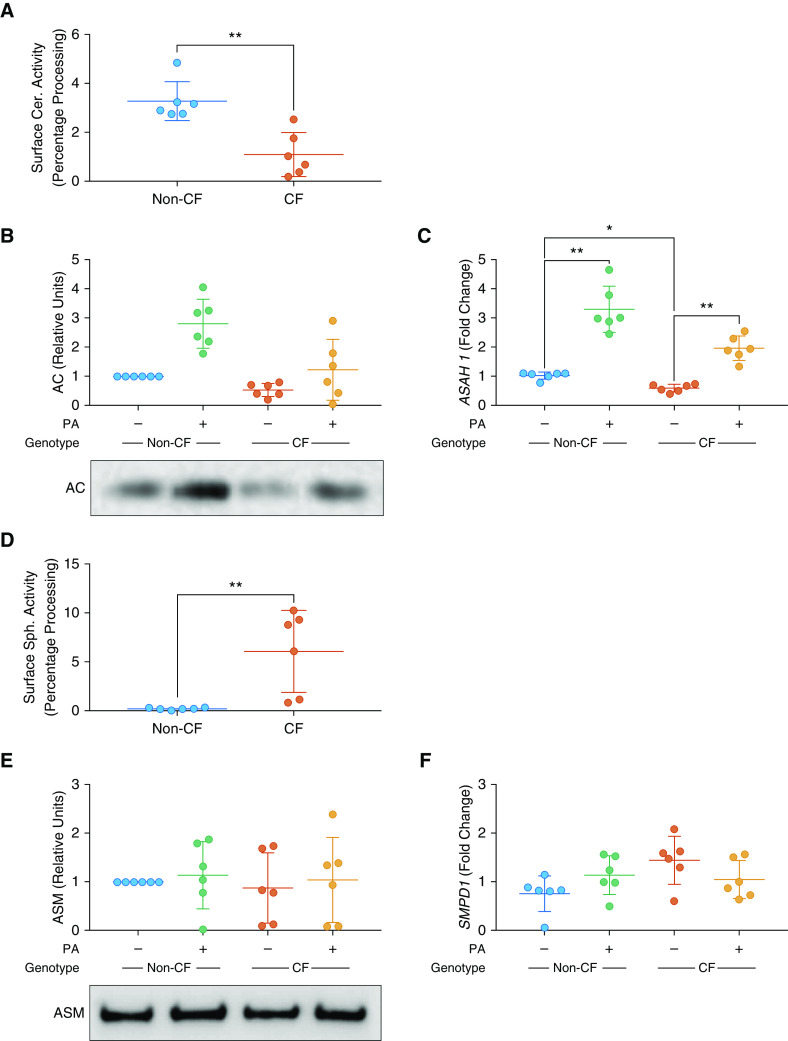
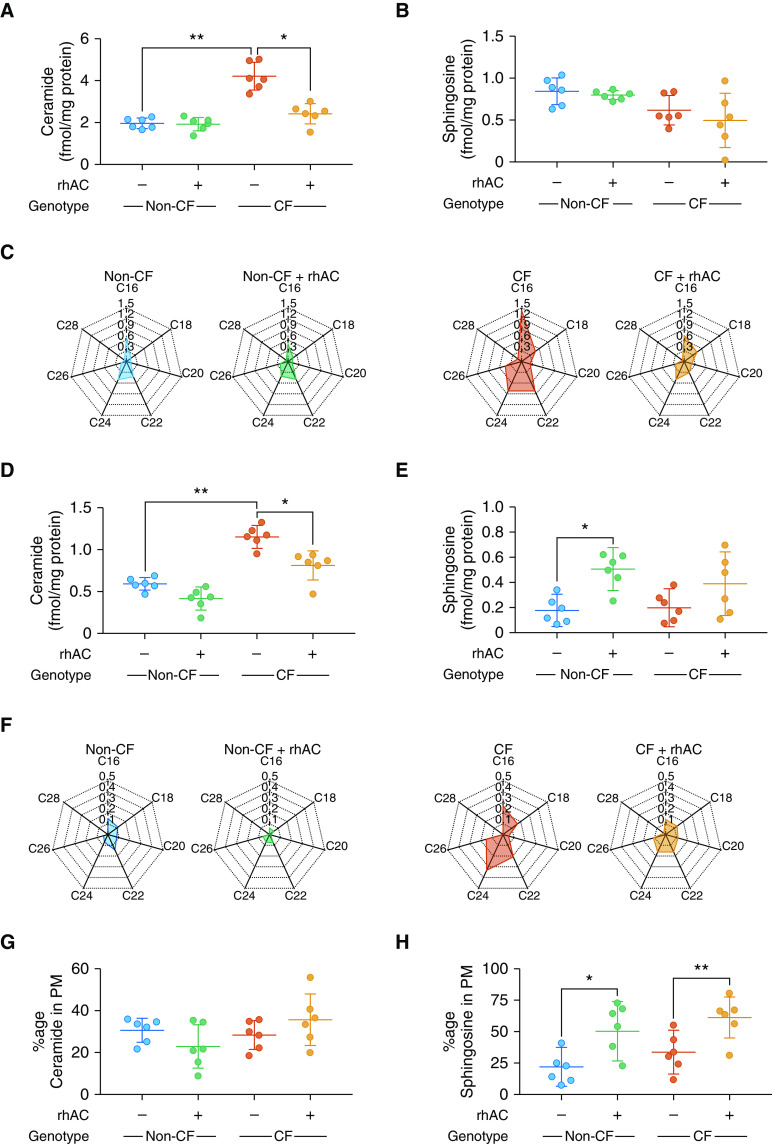
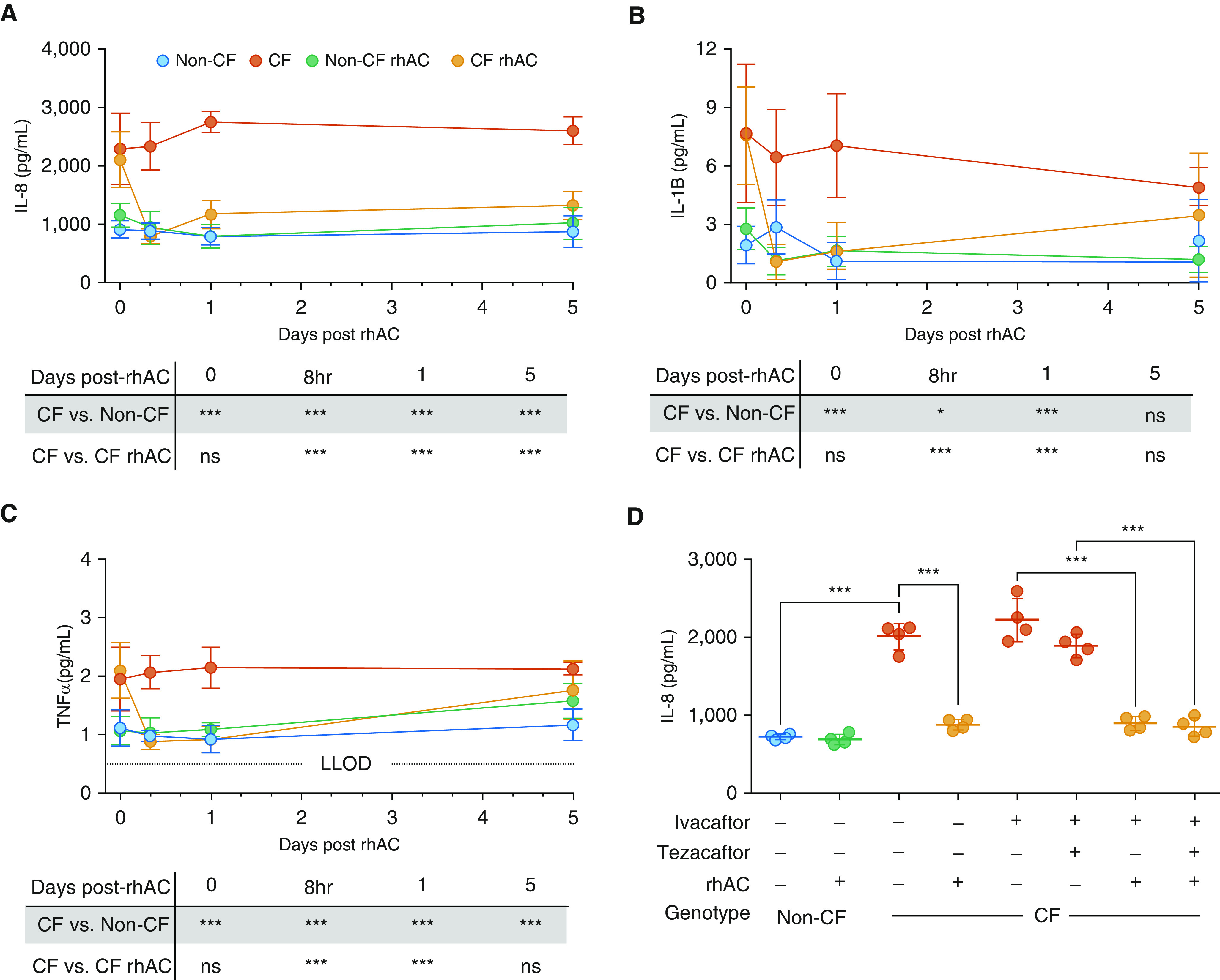
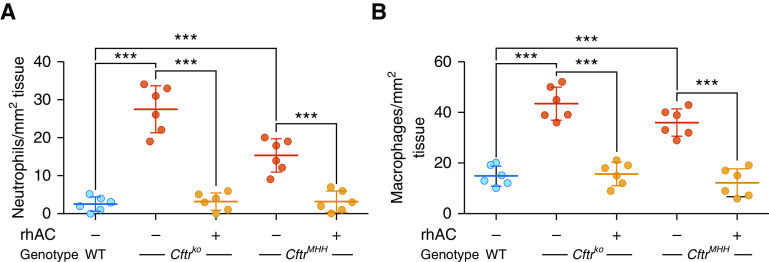
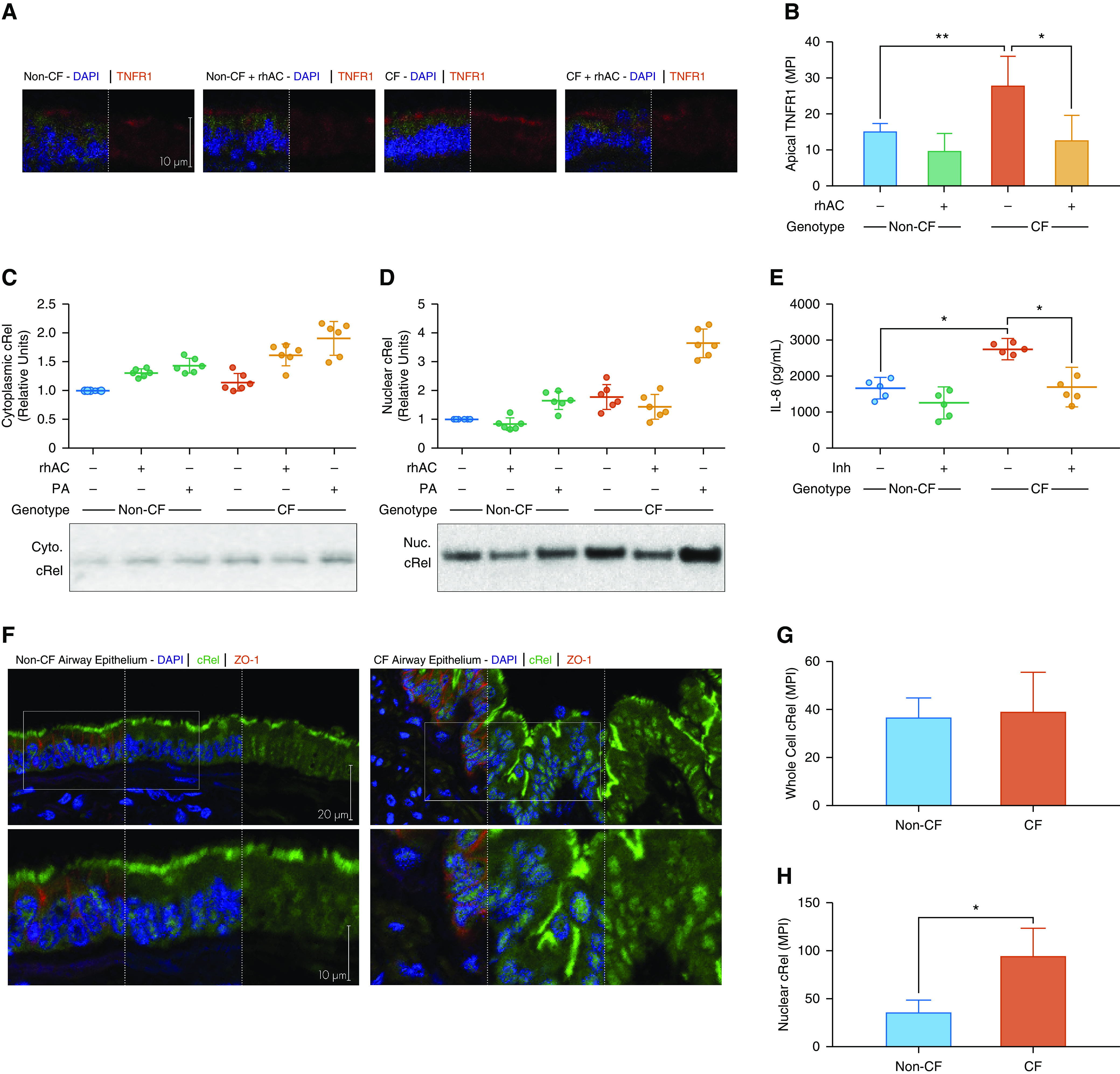
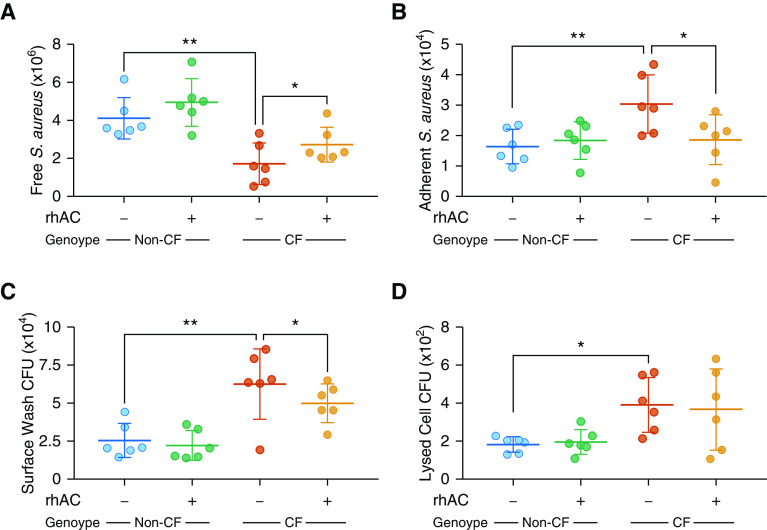
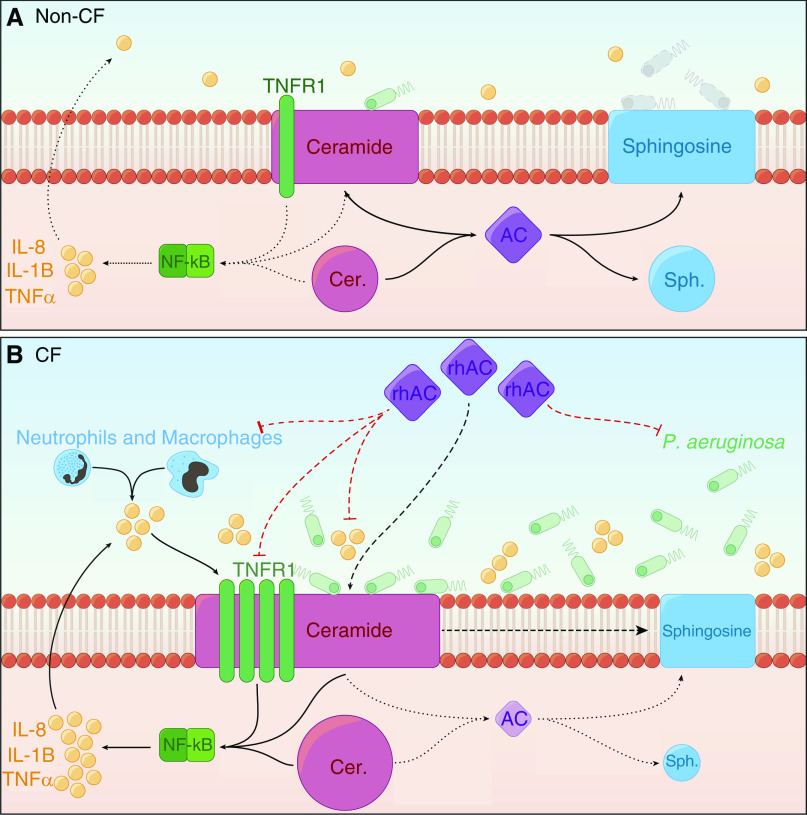
Rationale: In cystic fibrosis the major cause of morbidity and mortality is lung disease characterized by inflammation and infection. The influence of sphingolipid metabolism is poorly understood with a lack of studies using human airway model systems.Objectives: To investigate sphingolipid metabolism in cystic fibrosis and the effects of treatment with recombinant human acid ceramidase on inflammation and infection.Methods: Sphingolipids were measured using mass spectrometry in fully differentiated cultures of primary human airway epithelial cells and cocultures with Pseudomonas aeruginosa. In situ activity assays, Western blotting, and quantitative PCR were used to investigate function and expression of ceramidase and sphingomyelinase. Effects of treatment with recombinant human acid ceramidase on sphingolipid profile and inflammatory mediator production were assessed in cell cultures and murine models.Measurements and Main Results: Ceramide is increased in cystic fibrosis airway epithelium owing to differential function of enzymes regulating sphingolipid metabolism. Sphingosine, a metabolite of ceramide with antimicrobial properties, is not upregulated in response to P. aeruginosa by cystic fibrosis airway epithelia. Tumor necrosis factor receptor 1 is increased in cystic fibrosis epithelia and activates NF-κB signaling, generating inflammation. Treatment with recombinant human acid ceramidase, to decrease ceramide, reduced both inflammatory mediator production and susceptibility to infection.Conclusions: Sphingolipid metabolism is altered in airway epithelial cells cultured from people with cystic fibrosis. Treatment with recombinant acid ceramidase ameliorates the two pivotal features of cystic fibrosis lung disease, inflammation and infection, and thus represents a therapeutic approach worthy of further exploration.
Keywords: ceramide; lung; sphingolipid; sphingosine.
Figures
Comment in
-
Membrane Lipids and CFTR: The Yin/Yang of Efficient Ceramide Metabolism.Am J Respir Crit Care Med. 2020 Oct 15;202(8):1074-1075. doi: 10.1164/rccm.202006-2362ED. Am J Respir Crit Care Med. 2020. PMID: 32687399 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
