

Towards accurate exclusion of neonatal bacterial meningitis: a feasibility study of a novel 16S rDNA PCR assay
- PMID: 32571220
- PMCID: PMC7310343
- DOI: 10.1186/s12879-020-05160-x
Towards accurate exclusion of neonatal bacterial meningitis: a feasibility study of a novel 16S rDNA PCR assay
Abstract
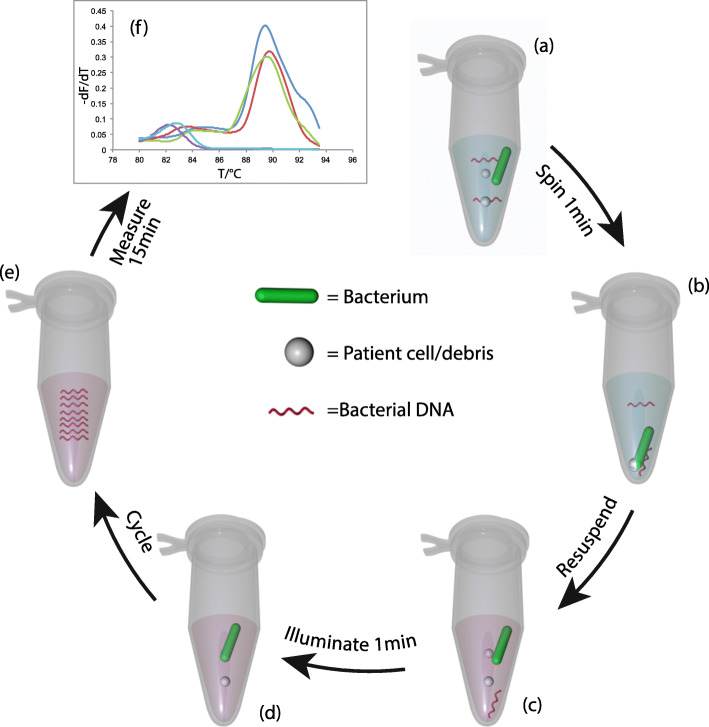
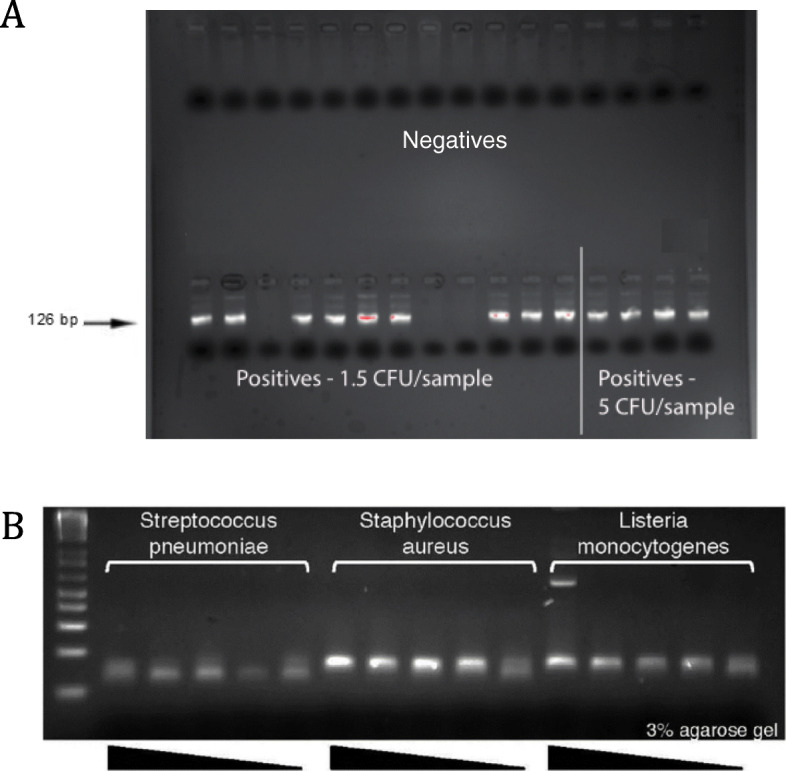
Background: PCRctic is an innovative assay based on 16S rDNA PCR technology that has been designed to detect a single intact bacterium in a specimen of cerebro-spinal fluid (CSF). The assay's potential for accurate, fast and inexpensive discrimination of bacteria-free CSF makes it an ideal adjunct for confident exclusion of bacterial meningitis in newborn babies where the negative predictive value of bacterial culture is poor. This study aimed to stress-test and optimize PCRctic in the "field conditions" to attain a clinically useful level of specificity.
Methods: The specificity of PCRctic was evaluated in CSF obtained from newborn babies investigated for meningitis on a tertiary neonatal unit. Following an interim analysis, the method of skin antisepsis was changed to increase bactericidal effect, and snap-top tubes (Eppendorf™) replaced standard universal containers for collection of CSF to reduce environmental contamination.
Results: The assay's specificity was 90.5% in CSF collected into the snap-top tubes - up from 60% in CSF in the universal containers. The method of skin antisepsis had no effect on the specificity. All CSF cultures were negative and no clinical cases of neonatal bacterial meningitis occurred during the study.
Conclusions: A simple and inexpensive optimization of CSF collection resulted in a high specificity output. The low prevalence of neonatal bacterial meningitis means that a large multi-centre study will be required to validate the assay's sensitivity and its negative predictive value.
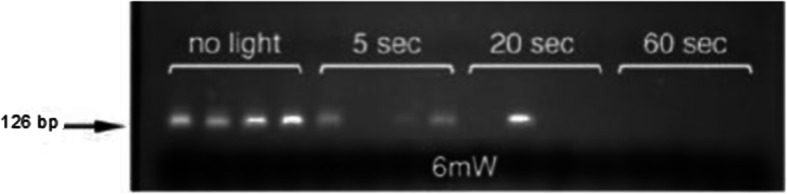
Keywords: Broad-range PCR; Ethidium monoazide; Neonatal bacterial meningitis.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Neonatal infection (early onset): antibiotics for prevention and treatment . National Institute for Health and Care Excellence Clinical Guideline 149. 2012.
-
- Kanegaye JT, Soliemanzadeh P, Bradley JS. Lumbar puncture in pediatric bacterial meningitis: determining the time interval for recovery of cerebrospinal fluid pathogens after parenteral antibiotic pretreatment. Pediatrics. 2001;108:1169–1174. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
