

Privacy-preserving architecture for providing feedback to clinicians on their clinical performance
- PMID: 32571306
- PMCID: PMC7310252
- DOI: 10.1186/s12911-020-01147-5
Privacy-preserving architecture for providing feedback to clinicians on their clinical performance
Abstract
Background: Learning from routine healthcare data is important for the improvement of the quality of care. Providing feedback on clinicians' performance in comparison to their peers has been shown to be more efficient for quality improvements. However, the current methods for providing feedback do not fully address the privacy concerns of stakeholders.
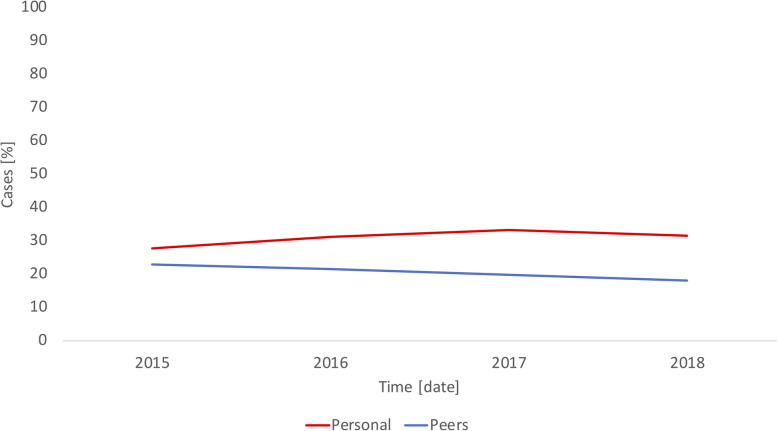
Methods: The paper proposes a distributed architecture for providing feedback to clinicians on their clinical performances while protecting their privacy. The indicators for the clinical performance of a clinician are computed within a healthcare institution based on pseudonymized data extracted from the electronic health record (EHR) system. Group-level indicators of clinicians across healthcare institutions are computed using privacy-preserving distributed data-mining techniques. A clinician receives feedback reports that compare his or her personal indicators with the aggregated indicators of the individual's peers. Indicators aggregated across different geographical levels are the basis for monitoring changes in the quality of care. The architecture feasibility was practically evaluated in three general practitioner (GP) offices in Norway that consist of about 20,245 patients. The architecture was applied for providing feedback reports to 21 GPs on their antibiotic prescriptions for selected respiratory tract infections (RTIs). Each GP received one feedback report that covered antibiotic prescriptions between 2015 and 2018, stratified yearly. We assessed the privacy protection and computation time of the architecture.
Results: Our evaluation indicates that the proposed architecture is feasible for practical use and protects the privacy of the patients, clinicians, and healthcare institutions. The architecture also maintains the physical access control of healthcare institutions over the patient data. We sent a single feedback report to each of the 21 GPs. A total of 14,396 cases were diagnosed with the selected RTIs during the study period across the institutions. Of these cases, 2924 (20.3%) were treated with antibiotics, where 40.8% (1194) of the antibiotic prescriptions were narrow-spectrum antibiotics.
Conclusions: It is feasible to provide feedback to clinicians on their clinical performance in comparison to peers across healthcare institutions while protecting privacy. The architecture also enables monitoring changes in the quality of care following interventions.
Keywords: Antibiotic prescriptions; Feedback; Learning healthcare system; Peer comparison, privacy; Quality improvement; Security.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures



Similar articles
-
A Privacy-Preserving Audit and Feedback System for the Antibiotic Prescribing of General Practitioners: Survey Study.JMIR Form Res. 2022 Jul 13;6(7):e31650. doi: 10.2196/31650. JMIR Form Res. 2022. PMID: 35830221 Free PMC article.
-
Can antibiotic prescriptions in respiratory tract infections be improved? A cluster-randomized educational intervention in general practice--the Prescription Peer Academic Detailing (Rx-PAD) Study [NCT00272155].BMC Health Serv Res. 2006 Jun 15;6:75. doi: 10.1186/1472-6963-6-75. BMC Health Serv Res. 2006. PMID: 16776824 Free PMC article.
-
Distributed clinical data sharing via dynamic access-control policy transformation.Int J Med Inform. 2016 May;89:25-31. doi: 10.1016/j.ijmedinf.2016.02.002. Epub 2016 Feb 12. Int J Med Inform. 2016. PMID: 26980356
-
Efficient Privacy-Preserving Access Control Scheme in Electronic Health Records System.Sensors (Basel). 2018 Oct 18;18(10):3520. doi: 10.3390/s18103520. Sensors (Basel). 2018. PMID: 30340411 Free PMC article.
-
Ending the Document Game: Connecting and Transforming Your Healthcare Through Information Technology [Internet].Bethesda (MD): National Library of Medicine (US); 2005. Bethesda (MD): National Library of Medicine (US); 2005. PMID: 35107905 Free Books & Documents. Review.
Cited by
-
The Norwegian PraksisNett: a nationwide practice-based research network with a novel IT infrastructure.Scand J Prim Health Care. 2022 Jun;40(2):217-226. doi: 10.1080/02813432.2022.2073966. Epub 2022 May 13. Scand J Prim Health Care. 2022. PMID: 35549798 Free PMC article.
-
A Privacy-Preserving Audit and Feedback System for the Antibiotic Prescribing of General Practitioners: Survey Study.JMIR Form Res. 2022 Jul 13;6(7):e31650. doi: 10.2196/31650. JMIR Form Res. 2022. PMID: 35830221 Free PMC article.
-
Automated extraction of standardized antibiotic resistance and prescription data from laboratory information systems and electronic health records: a narrative review.Front Antibiot. 2024 Mar 8;3:1380380. doi: 10.3389/frabi.2024.1380380. eCollection 2024. Front Antibiot. 2024. PMID: 39816258 Free PMC article. Review.
References
-
- Institute of Medicine (US) Roundtable on Evidence-Based Medicine. The Learning Healthcare System: Workshop Summary. Washington (DC): National Academies Press (US); 2007. http://www.ncbi.nlm.nih.gov/books/NBK53494/. Accessed 17 Nov 2015. - PubMed
-
- Institute of Medicine (US) and National Academy of Engineering (US) Roundtable on Value & Science-Driven Health Care. Engineering a Learning Healthcare System: A Look at the Future: Workshop Summary. Washington (DC): National Academies Press (US); 2011. http://www.ncbi.nlm.nih.gov/books/NBK61965/. Accessed 18 Nov 2015. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
