

A systematic review of pathological findings in COVID-19: a pathophysiological timeline and possible mechanisms of disease progression
- PMID: 32572155
- PMCID: PMC7306927
- DOI: 10.1038/s41379-020-0603-3
A systematic review of pathological findings in COVID-19: a pathophysiological timeline and possible mechanisms of disease progression
Abstract
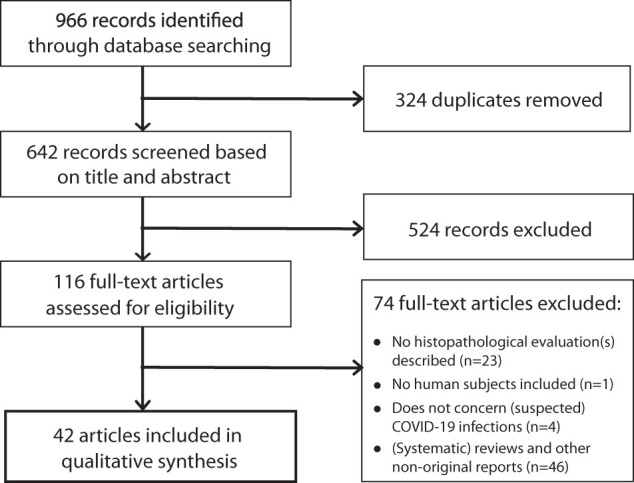
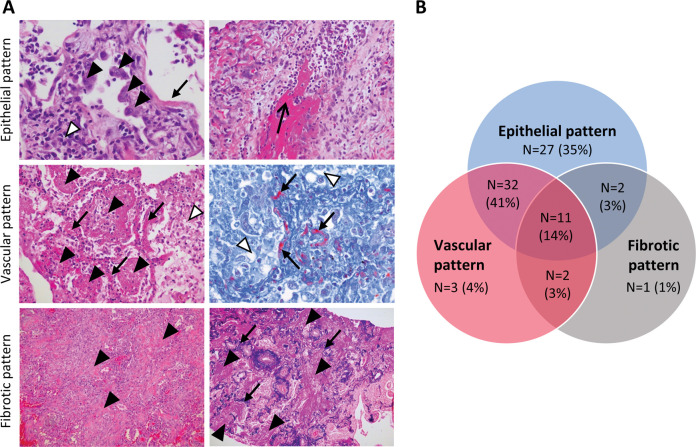
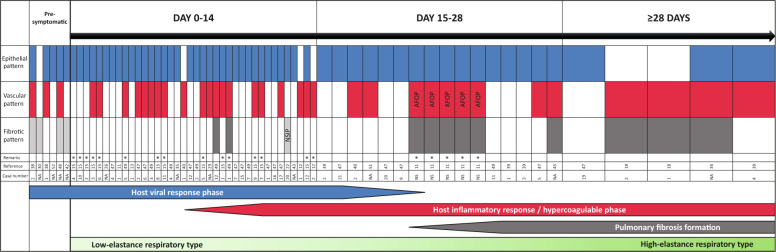
Since the outbreak of the COVID-19 pandemic, much has been learned regarding its clinical course, prognostic inflammatory markers, disease complications, and mechanical ventilation strategy. Clinically, three stages have been identified based on viral infection, pulmonary involvement with inflammation, and fibrosis. Moreover, low and high elastance phenotypes can be distinguished in mechanically ventilated patients, based on lung mechanics, ventilation-to-perfusion ratio, and CT scans; these two phenotypes have presumed differences in their underlying pathophysiology. Although essential for therapeutic guidance, the pathophysiology of COVID-19 is poorly understood. Here, we systematically reviewed published case reports and case series in order to increase our understanding of COVID-19 pathophysiology by constructing a timeline and correlating histopathological findings with clinical stages of COVID-19. Using PRISMA-IPD guidelines, 42 articles reporting 198 individual cases were included in our analysis. In lung samples (n = 131 cases), we identified three main histological patterns: epithelial (n = 110, 85%), with reactive epithelial changes and DAD; vascular (n = 76, 59%) with microvascular damage, (micro)thrombi, and acute fibrinous and organizing pneumonia; and fibrotic (n = 28, 22%) with interstitial fibrosis. The epithelial and vascular patterns can present in all stages of symptomatic COVID-19, whereas the fibrotic pattern presents starting at ~3 weeks. Moreover, patients can present with more than one pattern, either simultaneously or consecutively. These findings are consistent with knowledge regarding clinical patterns of viral infection, development of hyperinflammation and hypercoagulability, and fibrosis. Close collaboration among medical staff is necessary in order to translate this knowledge and classification of pathophysiological mechanisms into clinical stages of disease in individual patients. Moreover, further research, including histopathological studies, is warranted in order to develop reliable, clinically relevant biomarkers by correlating these pathological findings with laboratory results and radiological findings, thus, increasing our understanding of COVID-19 and facilitating the move to precision medicine for treating patients.
Figures
Comment in
-
Comments to: A systematic review of pathological findings in COVID-19: a pathophysiological timeline and possible mechanisms of disease progression.Mod Pathol. 2021 Aug;34(8):1608-1609. doi: 10.1038/s41379-020-0631-z. Epub 2020 Jul 21. Mod Pathol. 2021. PMID: 32694615 Free PMC article. No abstract available.
References
-
- WHO Director-General's remarks at the media briefing on 2019-nCoV on 11 February 2020 2020 [Internet] [cited April 22, 2020]: https://www.who.int/dg/speeches/detail/who-director-general-s-remarks-at....
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
