

The histologic presentation of hepatitis E reflects patients' immune status and pre-existing liver condition
- PMID: 32572157
- PMCID: PMC7806507
- DOI: 10.1038/s41379-020-0593-1
The histologic presentation of hepatitis E reflects patients' immune status and pre-existing liver condition
Abstract
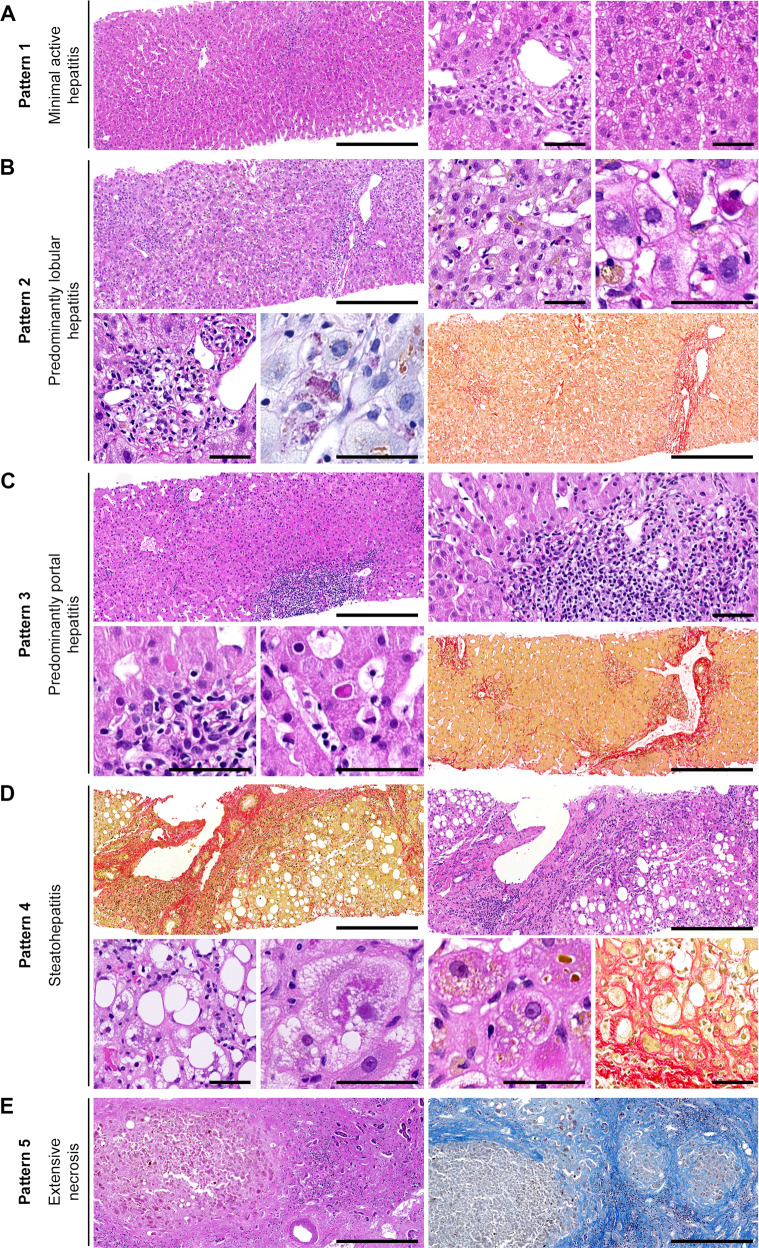
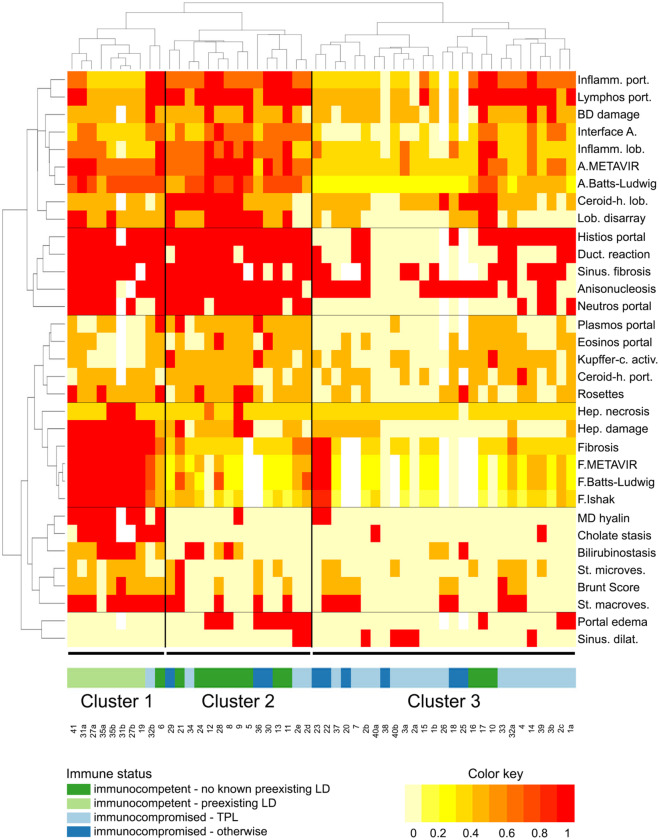
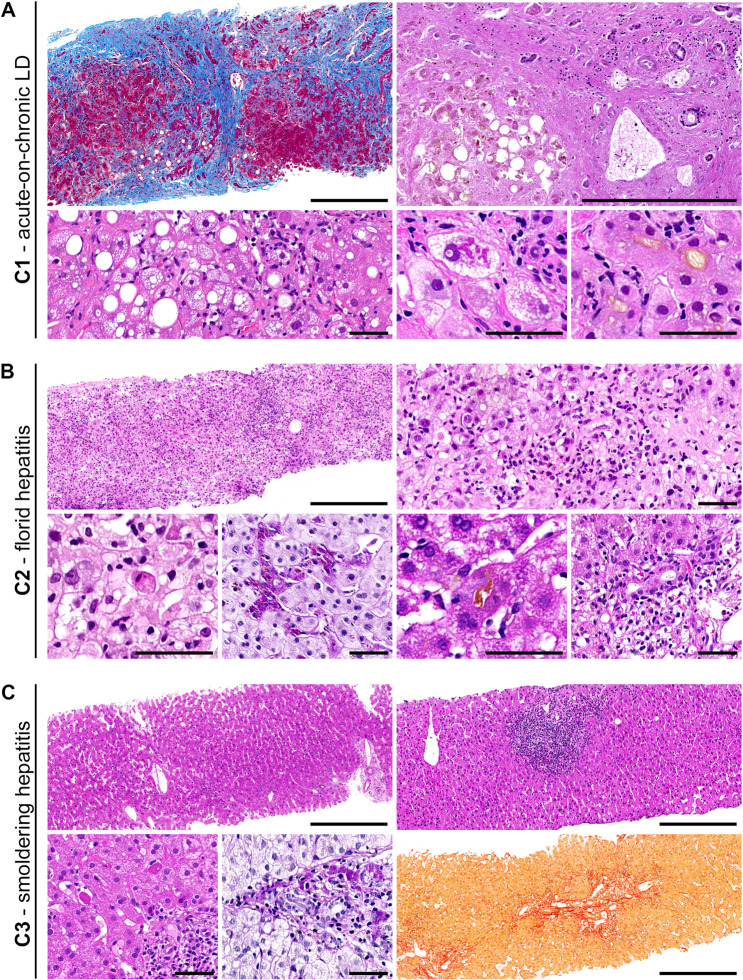
Infection with the hepatitis E virus (HEV) is one of the main causes of acute hepatitis worldwide. Given that, the histopathology of hepatitis E is relatively poorly characterized, and it is unclear what exactly determines its remarkable variability. The aim of our study was a systematic analysis of hepatitis E histology, especially with regard to the clinical setting. Fifty-two liver samples (48 biopsies, 1 liver explant, 3 autopsy livers) from 41 patients with molecularly proven hepatitis E (28 HEV genotype (gt) 3, three gt 1, one gt 4 and 9 undetermined gt) were systematically evaluated for 33 histopathologic features. Following one approach, the biopsies were assigned to one of five generic histologic patterns. In another approach, they were subjected to hierarchical clustering. We found that 23/41 (56%) patients were immunocompromised, whereas 18 (44%) had no known immunosuppression. Five patients (12%) had pre-existing liver disease (LD). The histopathologic spectrum ranged from almost normal to acute, chronic, and steato-hepatitis to subtotal necrosis, and was thus distributed across all five generic patterns. Hierarchical clustering, however, identified three histopathologic clusters (C1-C3), which segregated along the immune status and pre-existing LD: C1 comprised mostly patients with pre-existing LD; histology mainly reflected the respective LD without pointing to the additional hepatitis E. C2 comprised mostly immunocompetent patients; histology mainly displayed florid hepatitis. C3 comprised mostly immunocompromised patients; histology mainly displayed smoldering hepatitis. Accordingly, C1-C3 differed markedly with respect to their clinical and histopathologic differential diagnoses. Hierarchical clustering suggests three groups with distinct histopathologies, indicating biologically different manifestations of hepatitis E. The association of histopathologic changes with the patient's immune status and pre-existing LD plausibly explains the diversity of hepatitis E histopathology, and suggests that these factors are the crucial underlying determinants. We expect our results to improve patient management by guiding the clinico-pathologic diagnosis of hepatitis E.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures

References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
