

Multiple sclerosis lesions in motor tracts from brain to cervical cord: spatial distribution and correlation with disability
- PMID: 32572488
- PMCID: PMC7364770
- DOI: 10.1093/brain/awaa162
Multiple sclerosis lesions in motor tracts from brain to cervical cord: spatial distribution and correlation with disability
Abstract
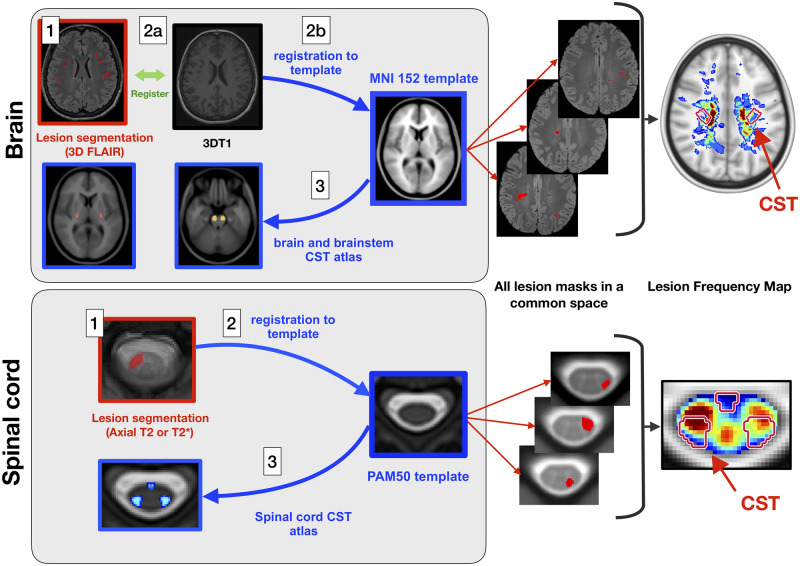
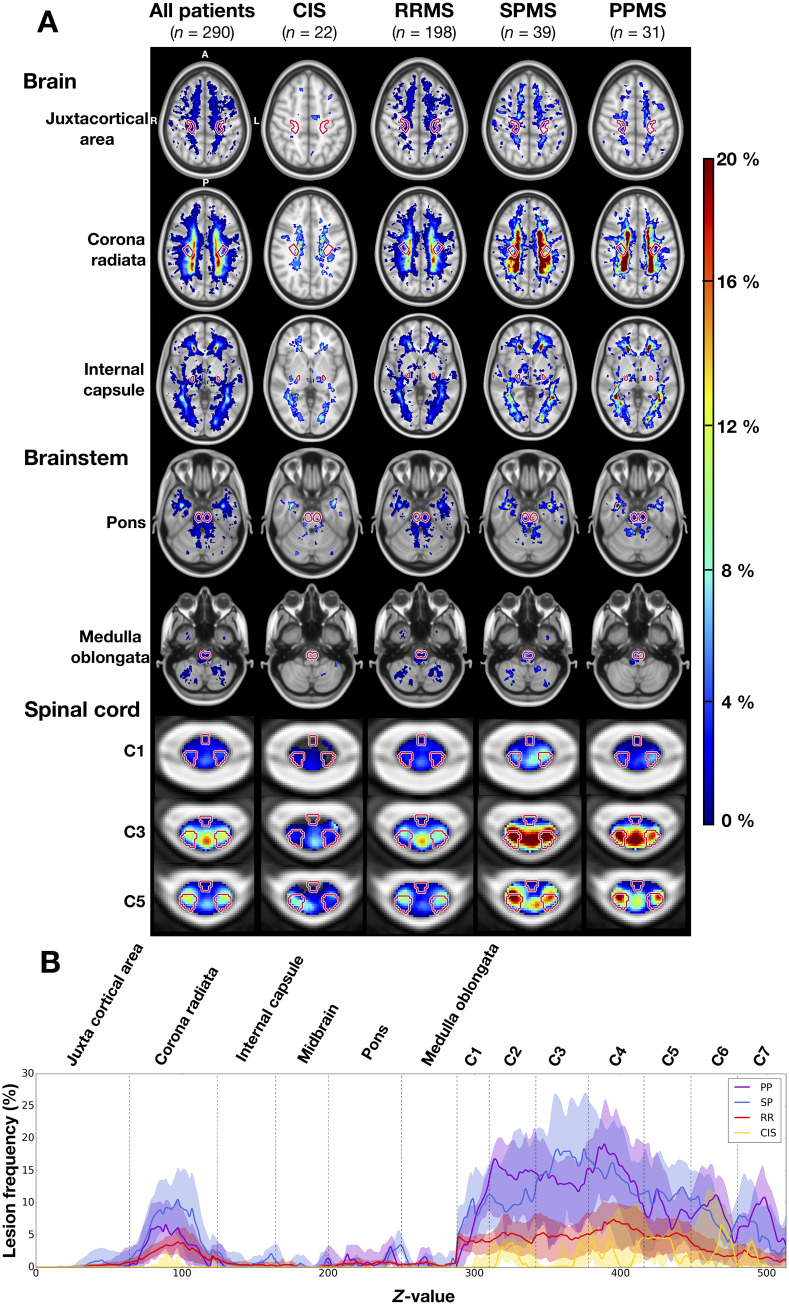
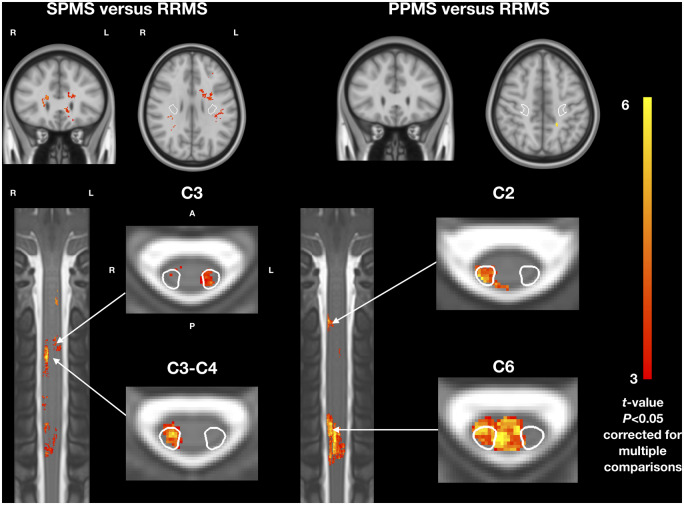
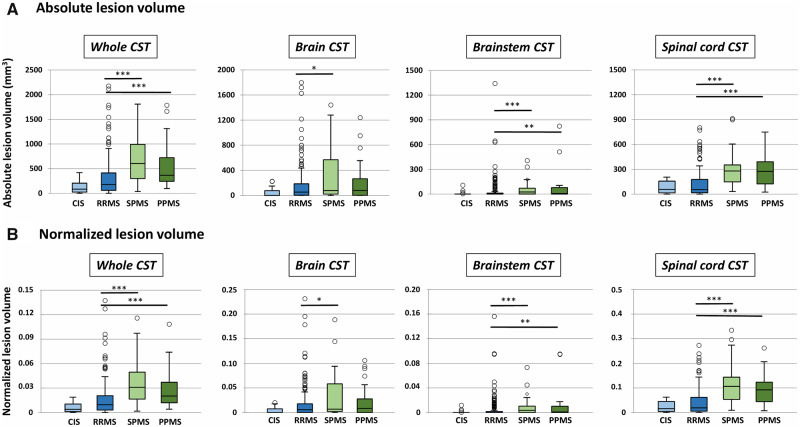
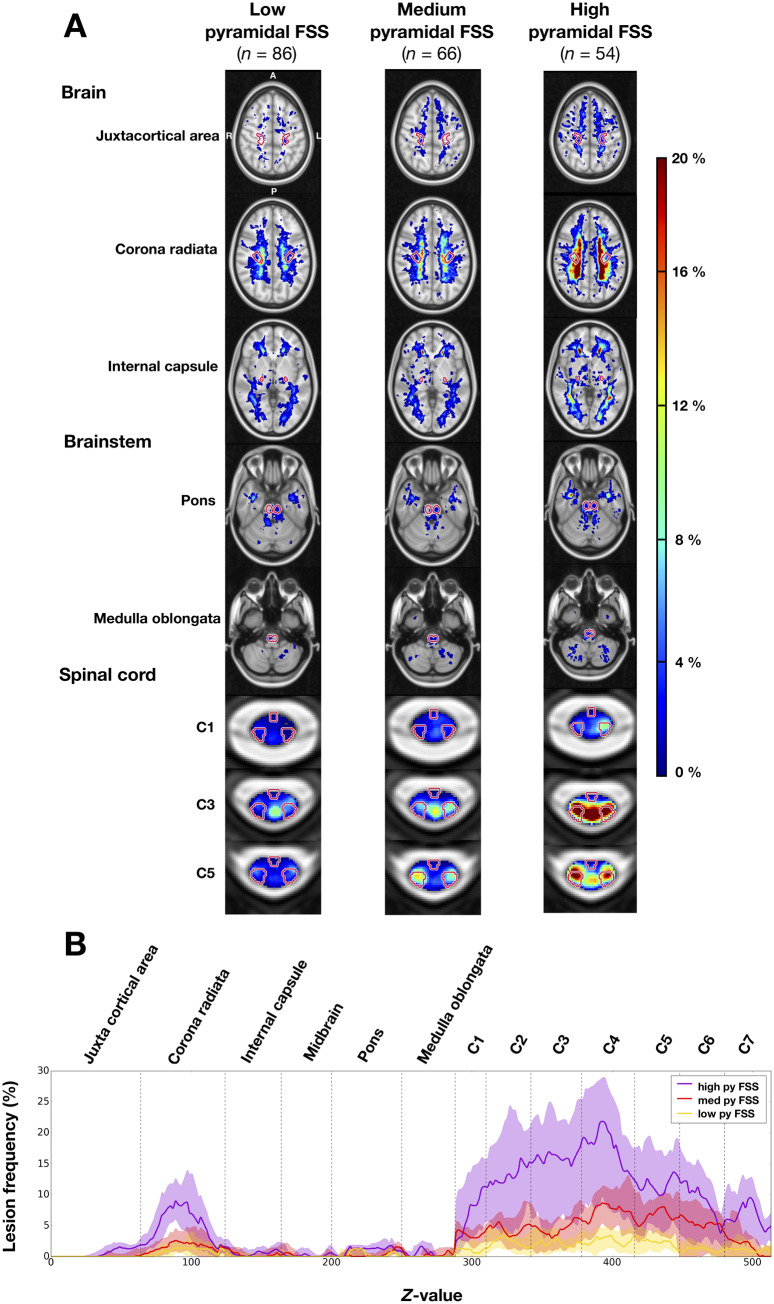
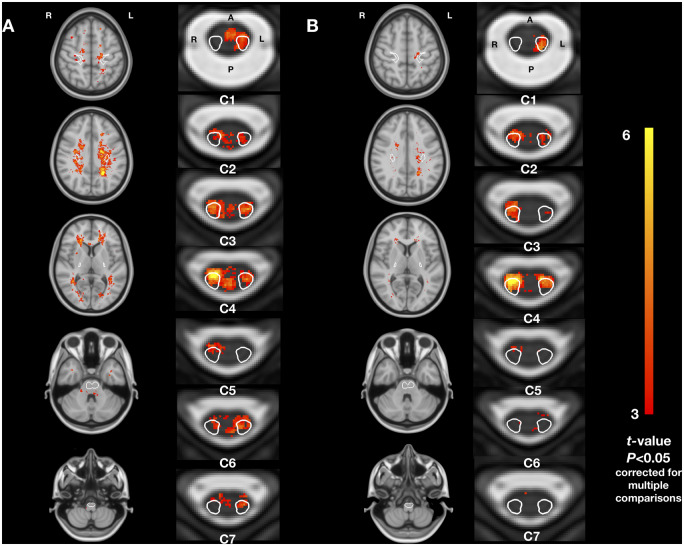
Despite important efforts to solve the clinico-radiological paradox, correlation between lesion load and physical disability in patients with multiple sclerosis remains modest. One hypothesis could be that lesion location in corticospinal tracts plays a key role in explaining motor impairment. In this study, we describe the distribution of lesions along the corticospinal tracts from the cortex to the cervical spinal cord in patients with various disease phenotypes and disability status. We also assess the link between lesion load and location within corticospinal tracts, and disability at baseline and 2-year follow-up. We retrospectively included 290 patients (22 clinically isolated syndrome, 198 relapsing remitting, 39 secondary progressive, 31 primary progressive multiple sclerosis) from eight sites. Lesions were segmented on both brain (T2-FLAIR or T2-weighted) and cervical (axial T2- or T2*-weighted) MRI scans. Data were processed using an automated and publicly available pipeline. Brain, brainstem and spinal cord portions of the corticospinal tracts were identified using probabilistic atlases to measure the lesion volume fraction. Lesion frequency maps were produced for each phenotype and disability scores assessed with Expanded Disability Status Scale score and pyramidal functional system score. Results show that lesions were not homogeneously distributed along the corticospinal tracts, with the highest lesion frequency in the corona radiata and between C2 and C4 vertebral levels. The lesion volume fraction in the corticospinal tracts was higher in secondary and primary progressive patients (mean = 3.6 ± 2.7% and 2.9 ± 2.4%), compared to relapsing-remitting patients (1.6 ± 2.1%, both P < 0.0001). Voxel-wise analyses confirmed that lesion frequency was higher in progressive compared to relapsing-remitting patients, with significant bilateral clusters in the spinal cord corticospinal tracts (P < 0.01). The baseline Expanded Disability Status Scale score was associated with lesion volume fraction within the brain (r = 0.31, P < 0.0001), brainstem (r = 0.45, P < 0.0001) and spinal cord (r = 0.57, P < 0.0001) corticospinal tracts. The spinal cord corticospinal tracts lesion volume fraction remained the strongest factor in the multiple linear regression model, independently from cord atrophy. Baseline spinal cord corticospinal tracts lesion volume fraction was also associated with disability progression at 2-year follow-up (P = 0.003). Our results suggest a cumulative effect of lesions within the corticospinal tracts along the brain, brainstem and spinal cord portions to explain physical disability in multiple sclerosis patients, with a predominant impact of intramedullary lesions.
Keywords: MRI; corticospinal tract; disability; multiple sclerosis.
© The Author(s) (2020). Published by Oxford University Press on behalf of the Guarantors of Brain. All rights reserved. For permissions, please email: journals.permissions@oup.com.
Figures
References
-
- Agosta F, Pagani E, Caputo D, Filippi M.. Associations between cervical cord gray matter damage and disability in patients with multiple sclerosis. Arch Neurol 2007; 64: 1302–5. - PubMed
-
- Arrambide G, Rovira A, Sastre-Garriga J, Tur C, Castilló J, Río J, et al.Spinal cord lesions: a modest contributor to diagnosis in clinically isolated syndromes but a relevant prognostic factor. Mult Scler 2018; 24: 301–12. - PubMed
-
- Barkhof F. The clinico-radiological paradox in multiple sclerosis revisited. Curr Opin Neurol 2002; 15: 239–45. - PubMed
