

Limb salvage procedure in immunocompromised patients with therapy-resistant leg ulcers-The value of ultra-radical debridement and instillation negative-pressure wound therapy
- PMID: 32573103
- PMCID: PMC7948940
- DOI: 10.1111/iwj.13428
Limb salvage procedure in immunocompromised patients with therapy-resistant leg ulcers-The value of ultra-radical debridement and instillation negative-pressure wound therapy
Abstract
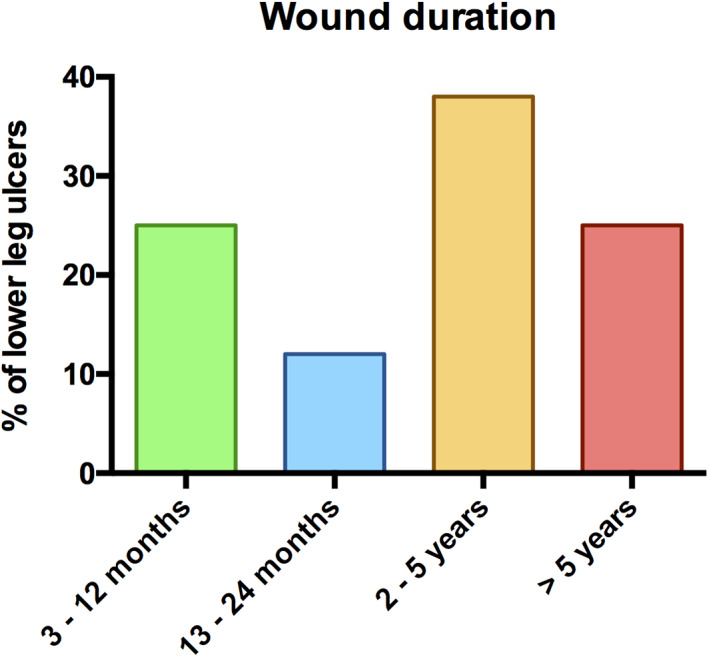
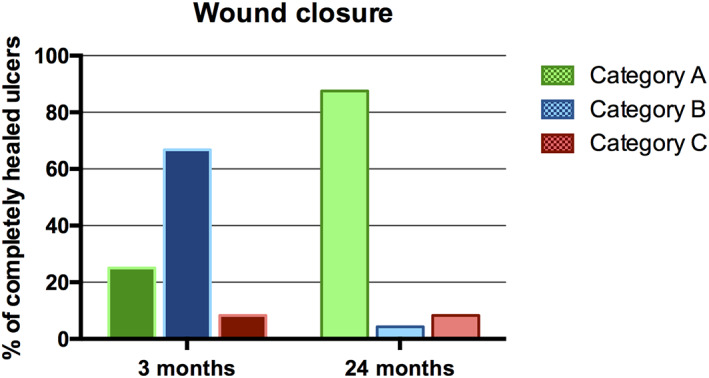
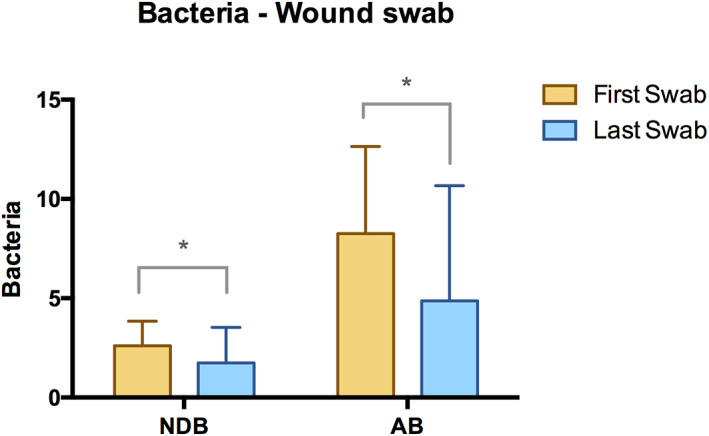
The purpose of this study was to analyse the outcome of our established triple treatment strategy in therapy-resistant deep-thickness chronic lower leg ulcers. This limb salvage approach consists of ultra-radical surgical debridement, negative-pressure wound therapy (NPWT) with or without instillation, and split-thickness skin grafting. Between March 2003 and December 2019, a total of 16 patients and 24 severe cases of lower leg ulcers were eligible for inclusion in this highly selective population. A total of seven patients received immunosuppressive medication. Complete wound closure was achieved in 25% and almost 90% of included lower leg ulcer cases after 3 and 24 months of our triple treatment strategy, respectively. The overall limb salvage rate was 100%. Bacterial colonisation of these wounds was significantly reduced after multiple surgical debridements and NPWT. Fasciotomy and radical removal of devitalised tissue such as deep fascia, tendons, and muscles combined with NPWT showed promising results in terms of the overall graft take rate. This treatment strategy was considered as last resort for limb salvage in such a critically ill and immunocompromised patient population. Surgeons should be aware of its efficacy and consider the triple treatment strategy especially if no other limb salvage option remains.
Keywords: chronic leg ulcer; negative-pressure wound therapy; skin transplantation; ultra-radical debridement.
© 2020 The Authors. International Wound Journal published by Medicalhelplines.com Inc and John Wiley & Sons Ltd.
Conflict of interest statement
R. E. H. has received third party funding for scientific research on NPWT from KCI—an Acelity company in the past and has served as a member of a Scientific Advisory Board of KCI‐Acelity in the past. R. E. H. and A. A. served as speakers on scientific symposia of KCI‐Acelity in the past. The authors have no other relevant affiliations or financial involvement with any organisation or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Figures


Similar articles
-
Coverage of exposed bones and joints in critically ill patients: lower extremity salvage with topical negative pressure therapy.J Cutan Med Surg. 2008 Sep-Oct;12(5):223-9. doi: 10.2310/7750.2008.07073. J Cutan Med Surg. 2008. PMID: 18845091
-
Comparing the Therapeutic Value of Negative Pressure Wound Therapy and Negative Pressure Wound Therapy With Instillation and Dwell Time in Bilateral Leg Ulcers: A Case Report.Wounds. 2019 Sep;31(9):E61-E64. Wounds. 2019. PMID: 31730514
-
[Surgical treatment for chronic leg ulcer].Hautarzt. 2020 Sep;71(9):715-723. doi: 10.1007/s00105-020-04661-9. Hautarzt. 2020. PMID: 32827047 German.
-
Wound care in venous ulcers.Phlebology. 2013 Mar;28 Suppl 1:79-85. doi: 10.1177/0268355513477015. Phlebology. 2013. PMID: 23482540 Review.
-
Sacral and Ischial Pressure Ulcer Management With Negative-Pressure Wound Therapy With Instillation and Dwell.Plast Reconstr Surg. 2021 Jan 1;147(1S-1):61S-67S. doi: 10.1097/PRS.0000000000007613. Plast Reconstr Surg. 2021. PMID: 33347064
Cited by
-
The Value of Negative-Pressure Wound Therapy and Flap Surgery in Hidradenitis Suppurativa - A Single Center Analysis of Different Treatment Options.Front Surg. 2022 Jun 28;9:867487. doi: 10.3389/fsurg.2022.867487. eCollection 2022. Front Surg. 2022. PMID: 35836613 Free PMC article.
-
Natural products in the treatment of diabetic foot infection.Eur J Med Res. 2025 Jan 7;30(1):8. doi: 10.1186/s40001-024-02255-y. Eur J Med Res. 2025. PMID: 39773682 Free PMC article. Review.
-
Effects of Different Pressure Levels in Topical Negative Pressure Application-Analysis of Perfusion Parameters in a Clinical Skin Model Using Multimodal Imaging Techniques.J Clin Med. 2022 Aug 31;11(17):5133. doi: 10.3390/jcm11175133. J Clin Med. 2022. PMID: 36079063 Free PMC article.
-
Is Instillational Topical Negative Pressure Wound Therapy in Peri-Prosthetic Infections of the Breast Effective? A Pilot Study.J Pers Med. 2022 Dec 13;12(12):2054. doi: 10.3390/jpm12122054. J Pers Med. 2022. PMID: 36556274 Free PMC article.
-
[Reconstruction of oncological defects of the perianal region].Chirurg. 2021 Dec;92(12):1159-1170. doi: 10.1007/s00104-021-01394-w. Epub 2021 Apr 27. Chirurg. 2021. PMID: 33904942 German.
References
-
- Briggs M, Closs SJ. The prevalence of leg ulceration: a review of the literature. EWMA J. 2003;3:14‐20.
-
- Rayner RCK, Carville K, Keaton J, Prentice J, Santamaria N. Leg ulcers: atypical presentations and associated comorbidities. Wound Pract Res. 2009;17:168‐184.
-
- Knighton DR, Fylling CP, Fiegel VD, Cerra F. Amputation prevention in an independently reviewed at‐risk diabetic population using a comprehensive wound care protocol. Am J Surg. 1990;160(5):466‐471. (Discussion 71‐72). - PubMed
-
- Körber A, Klode J, Al‐Benna S, et al. Etiology of chronic leg ulcers in 31,619 patients in Germany analyzed by an expert survey. J Ger Soc Dermatol. 2011;9(2):116‐121. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
