

SARS-CoV-2 infection of the placenta
- PMID: 32573498
- PMCID: PMC7456249
- DOI: 10.1172/JCI139569
SARS-CoV-2 infection of the placenta
Abstract
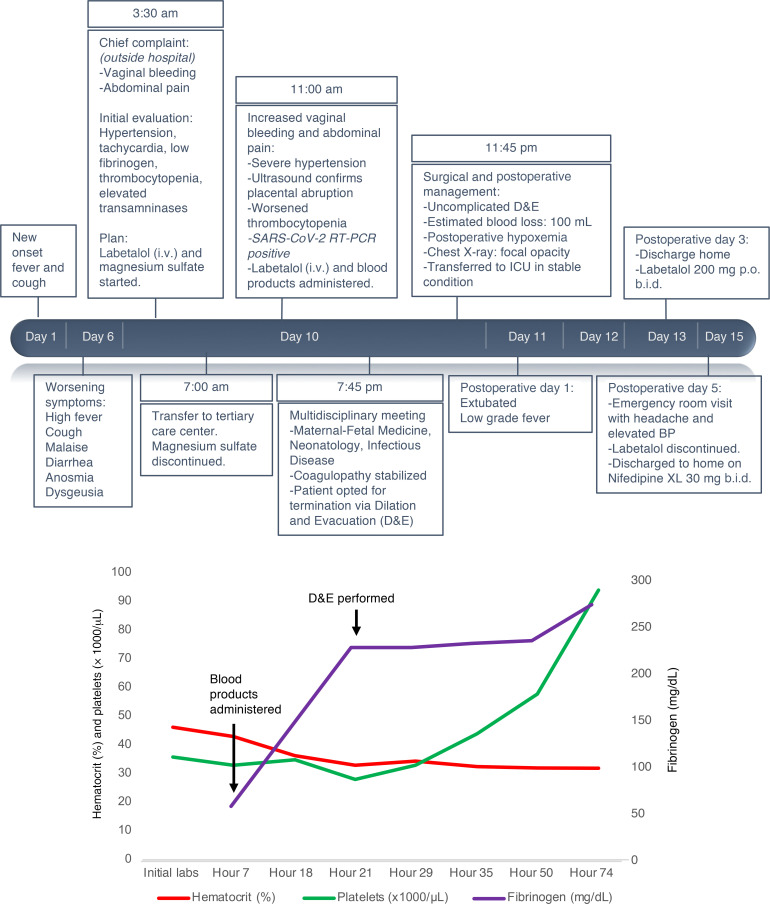
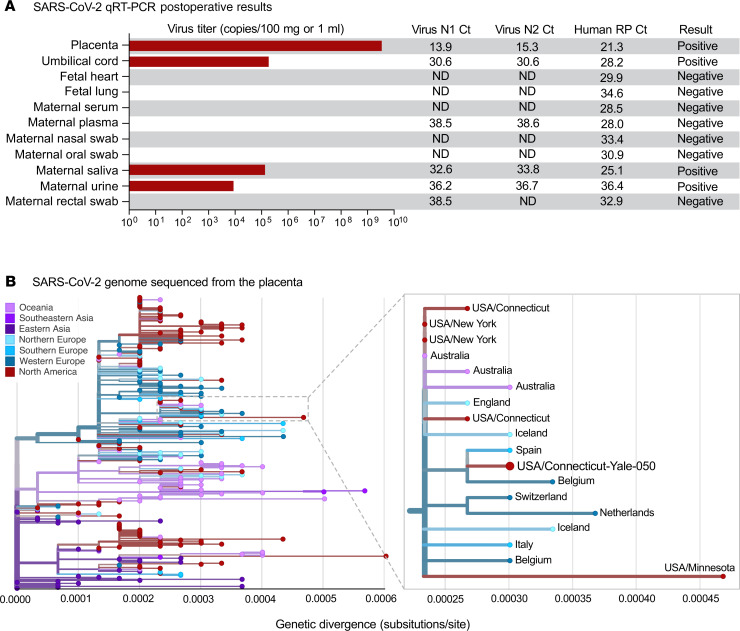
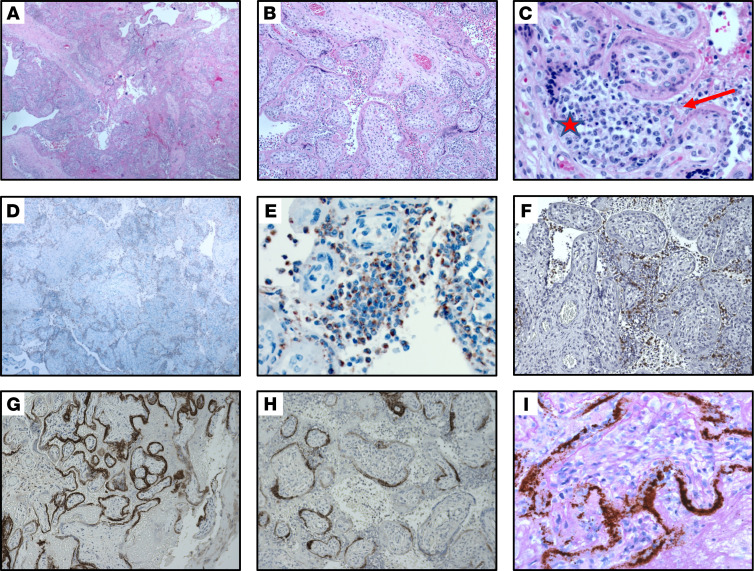
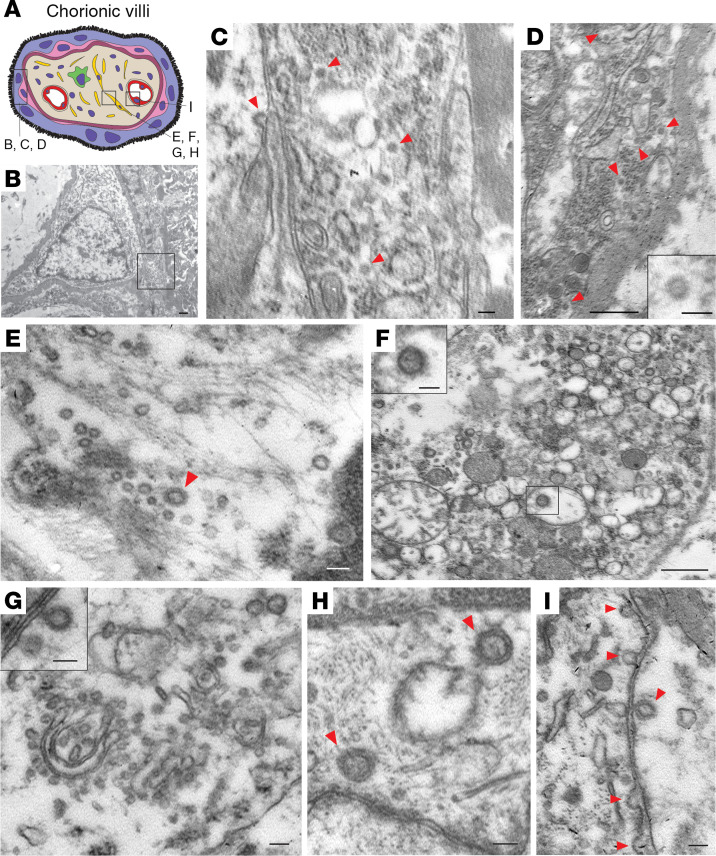
BACKGROUNDThe effects of the novel coronavirus disease 2019 (COVID-19) in pregnancy remain relatively unknown. We present a case of second trimester pregnancy with symptomatic COVID-19 complicated by severe preeclampsia and placental abruption.METHODSWe analyzed the placenta for the presence of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) through molecular and immunohistochemical assays and by and electron microscopy and measured the maternal antibody response in the blood to this infection.RESULTSSARS-CoV-2 localized predominantly to syncytiotrophoblast cells at the materno-fetal interface of the placenta. Histological examination of the placenta revealed a dense macrophage infiltrate, but no evidence for the vasculopathy typically associated with preeclampsia.CONCLUSIONThis case demonstrates SARS-CoV-2 invasion of the placenta, highlighting the potential for severe morbidity among pregnant women with COVID-19.FUNDINGBeatrice Kleinberg Neuwirth Fund and Fast Grant Emergent Ventures funding from the Mercatus Center at George Mason University. The funding bodies did not have roles in the design of the study or data collection, analysis, and interpretation and played no role in writing the manuscript.
Keywords: COVID-19; Molecular pathology; Reproductive Biology.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
