

Association of Perceived Stress Levels With Long-term Mortality in Patients With Peripheral Artery Disease
- PMID: 32573710
- PMCID: PMC7312389
- DOI: 10.1001/jamanetworkopen.2020.8741
Association of Perceived Stress Levels With Long-term Mortality in Patients With Peripheral Artery Disease
Abstract
Importance: Identifying modifiable risk factors, such as stress, that could inform the design of peripheral artery disease (PAD) management strategies is critical for reducing the risk of mortality. Few studies have examined the association of self-perceived stress with outcomes in patients with PAD.
Objective: To examine the association of high levels of self-perceived stress with mortality in patients with PAD.
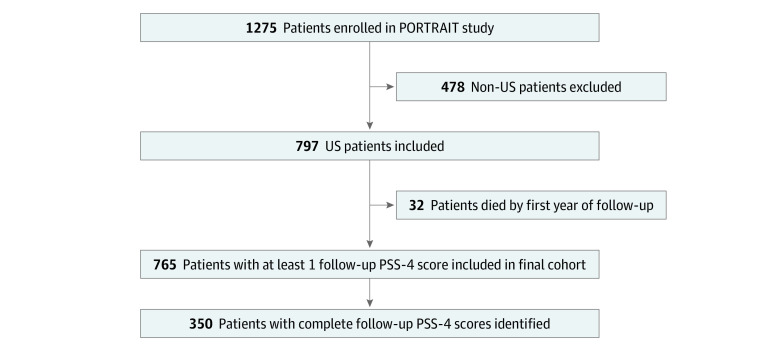
Design, setting, and participants: This cohort study analyzed data from the registry of the Patient-Centered Outcomes Related to Treatment Practices in Peripheral Arterial Disease: Investigating Trajectories (PORTRAIT) study, a multicenter study that enrolled patients with new or worsening symptoms of PAD who presented to 16 subspecialty clinics across the US, the Netherlands, and Australia from June 2, 2011, to December 3, 2015. However, the present study included only patients in the US sites because assessments of mortality for patients in the Netherlands and Australia were not available. Data analysis was conducted from July 2019 to March 2020.
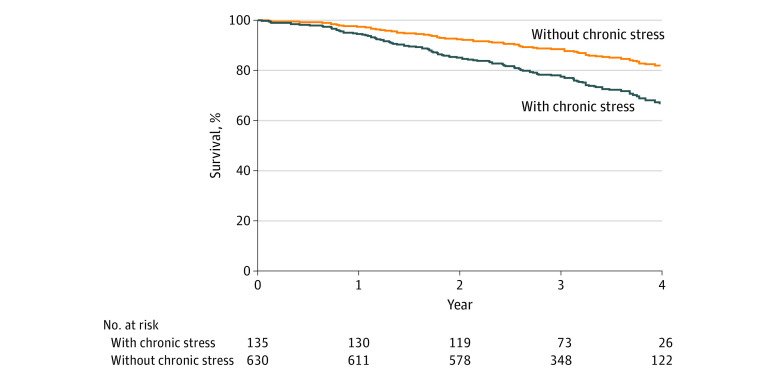
Exposure: Self-perceived stress was quantified using the 4-item Perceived Stress Scale (PSS-4), with a score range of 0 to 16. A score of 6 or higher indicated high stress in this cohort. Missing scores were imputed using multiple imputation by chained equations with predictive mean matching. Stress was assessed at baseline and at 3-, 6-, and 12-month follow-up. Patients who reported high levels of stress at 2 or more follow-up assessments were categorized as having chronic stress.
Main outcomes and measures: All-cause mortality was the primary study outcome. Such data for the subsequent 4 years after the 12-month follow-up were obtained from the National Death Index.
Results: The final cohort included 765 patients, with a mean (SD) age of 68.4 (9.7) years. Of these patients, 57.8% were men and 71.6% were white individuals. High stress levels were reported in 65% of patients at baseline and in 20% at the 12-month follow-up. In an adjusted Cox proportional hazards regression model accounting for demographics, comorbidities, disease severity, treatment type, and socioeconomic status, exposure to chronic stress during the 12 months of follow-up was independently associated with increased risk of all-cause mortality in the subsequent 4 years (hazard ratio, 2.12; 95% CI, 1.14-3.94; P = .02).
Conclusions and relevance: In thie cohort study of patients with PAD, higher stress levels in the year after diagnosis appeared to be associated with greater long-term mortality risk, even after adjustment for confounding factors. These findings suggest that, given that stress is a modifiable risk factor for which evidence-based management strategies exist, a holistic approach that includes assessment of chronic stress has the potential to improve survival in patients with PAD.
Conflict of interest statement
Figures
References
-
- Kalbaugh CA, Kucharska-Newton A, Wruck L, et al. . Peripheral artery disease prevalence and incidence estimated from both outpatient and inpatient settings among Medicare fee-for-service beneficiaries in the Atherosclerosis Risk in Communities (ARIC) study. J Am Heart Assoc. 2017;6(5):e003796. doi:10.1161/JAHA.116.003796 - DOI - PMC - PubMed
-
- Kalbaugh CA, Loehr L, Wruck L, et al. . Frequency of care and mortality following an incident diagnosis of peripheral artery disease in the inpatient or outpatient setting: the ARIC (Atherosclerosis Risk in Communities) study. J Am Heart Assoc. 2018;7(8):e007332. doi:10.1161/JAHA.117.007332 - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
