

Coronary vascular growth matches IGF-1-stimulated cardiac growth in fetal sheep
- PMID: 32573852
- PMCID: PMC7688557
- DOI: 10.1096/fj.202000215R
Coronary vascular growth matches IGF-1-stimulated cardiac growth in fetal sheep
Abstract
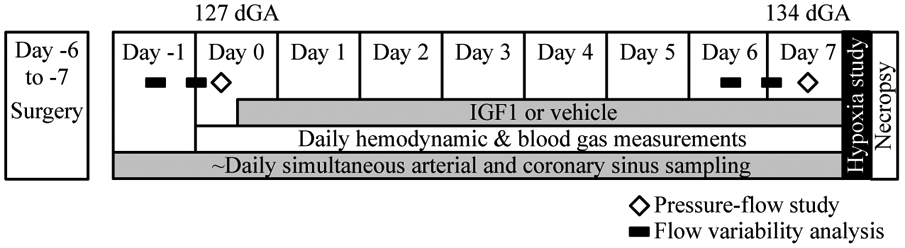
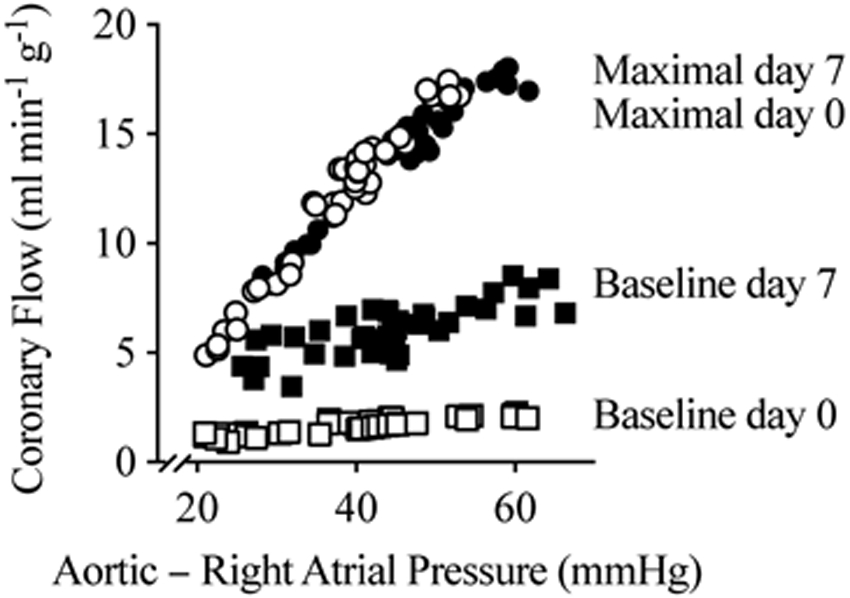
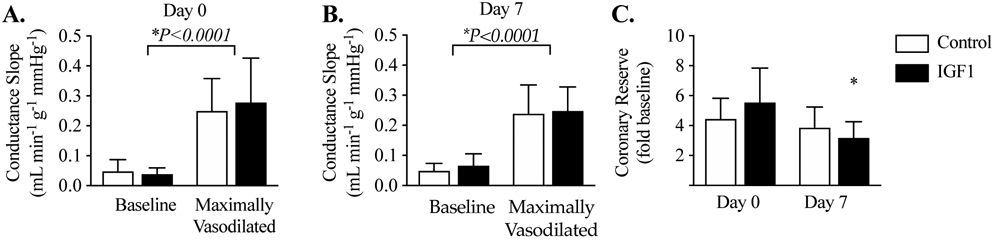
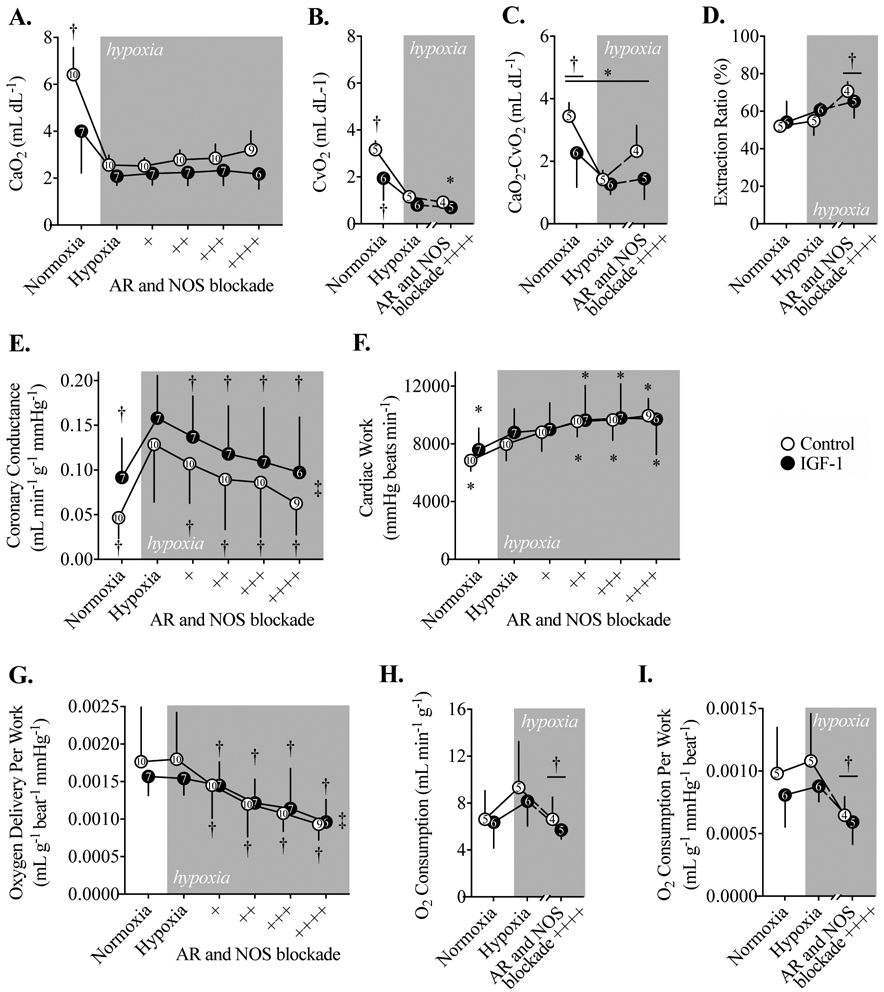
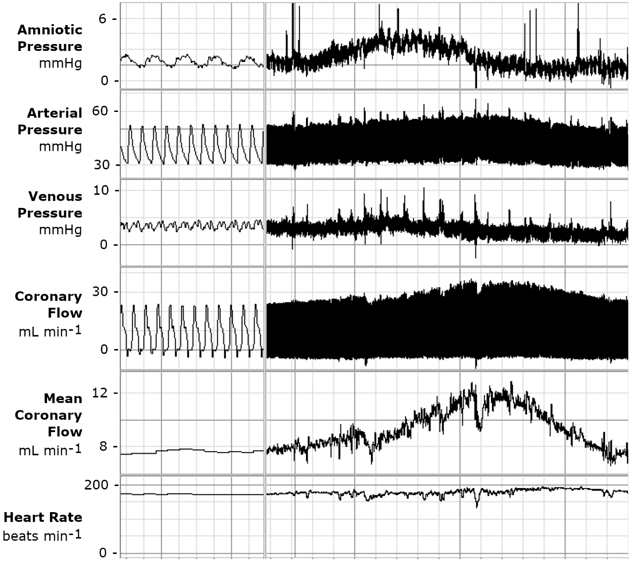
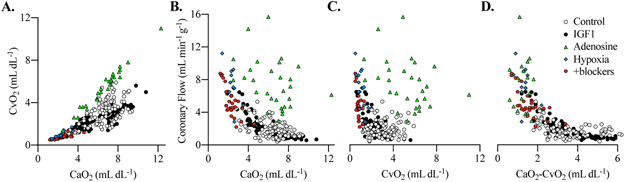
As loss of contractile function in heart disease could often be mitigated by increased cardiomyocyte number, expansion of cardiomyocyte endowment paired with increased vascular supply is a desirable therapeutic goal. Insulin-like growth factor 1 (IGF-1) administration increases fetal cardiomyocyte proliferation and heart mass, but how fetal IGF-1 treatment affects coronary growth and function is unknown. Near-term fetal sheep underwent surgical instrumentation and were studied from 127 to 134 d gestation (term = 147 d), receiving either IGF-1 LR3 or vehicle. Coronary growth and function were interrogated using pressure-flow relationships, an episode of acute hypoxia with progressive blockade of adenosine receptors and nitric oxide synthase, and by modeling the determinants of coronary flow. The main findings were that coronary conductance was preserved on a per-gram basis following IGF-1 treatment, adenosine and nitric oxide contributed to hypoxia-mediated coronary vasodilation similarly in IGF-1-treated and Control fetuses, and the relationships between coronary flow and blood oxygen contents were similar between groups. We conclude that IGF-1-stimulated fetal myocardial growth is accompanied by appropriate expansion and function of the coronary vasculature. These findings support IGF-1 as a potential strategy to increase cardiac myocyte and coronary vascular endowment at birth.
Keywords: adenosine; angiogenesis; contracture; coronary autoregulation; developmental origins; nitric oxide.
© 2020 Federation of American Societies for Experimental Biology.
Figures
References
-
- Benjamin EJ, Virani SS, Callaway CW, Chamberlain AM, Chang AR, Cheng S, Chiuve SE, Cushman M, Delling FN, Deo R, de Ferranti SD, Ferguson JF, Fornage M, Gillespie C, Isasi CR, Jimenez MC, Jordan LC, Judd SE, Lackland D, Lichtman JH, Lisabeth L, Liu S, Longenecker CT, Lutsey PL, Mackey JS, Matchar DB, Matsushita K, Mussolino ME, Nasir K, O’Flaherty M, Palaniappan LP, Pandey A, Pandey DK, Reeves MJ, Ritchey MD, Rodriguez CJ, Roth GA, Rosamond WD, Sampson UKA, Satou GM, Shah SH, Spartano NL, Tirschwell DL, Tsao CW, Voeks JH, Willey JZ, Wilkins JT, Wu JH, Alger HM, Wong SS, Muntner P, American Heart Association Council on, E., Prevention Statistics, C., and Stroke Statistics, S. (2018) Heart Disease and Stroke Statistics-2018 Update: A Report From the American Heart Association. Circulation 137, e67–e492 - PubMed
-
- Chien KR, Frisen J, Fritsche-Danielson R, Melton DA, Murry CE, and Weissman IL (2019) Regenerating the field of cardiovascular cell therapy. Nat. Biotechnol 37, 232–237 - PubMed
-
- Burrell JH, Boyn AM, Kumarasamy V, Hsieh A, Head SI, and Lumbers ER (2003) Growth and maturation of cardiac myocytes in fetal sheep in the second half of gestation. Anat. Rec. A Discov. Mol. Cell. Evol. Biol 274, 952–961 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
