

Association Between Arterial Carbon Dioxide Tension and Clinical Outcomes in Venoarterial Extracorporeal Membrane Oxygenation
- PMID: 32574466
- PMCID: PMC7393440
- DOI: 10.1097/CCM.0000000000004347
Association Between Arterial Carbon Dioxide Tension and Clinical Outcomes in Venoarterial Extracorporeal Membrane Oxygenation
Abstract
Objectives: The manipulation of arterial carbon dioxide tension is associated with differential mortality and neurologic injury in intensive care and cardiac arrest patients; however, few studies have investigated this relationship in patients on venoarterial extracorporeal membrane oxygenation. We investigated the association between the initial arterial carbon dioxide tension and change over 24 hours on mortality and neurologic injury in patients undergoing venoarterial extracorporeal membrane oxygenation for cardiac arrest and refractory cardiogenic shock.
Design: Retrospective cohort analysis of adult patients recorded in the international Extracorporeal Life Support Organization Registry.
Setting: Data reported to the Extracorporeal Life Support Organization from all international extracorporeal membrane oxygenation centers during 2003-2016.
Patients: Adult patients (≥ 18 yr old) supported with venoarterial extracorporeal membrane oxygenation.
Interventions: None.
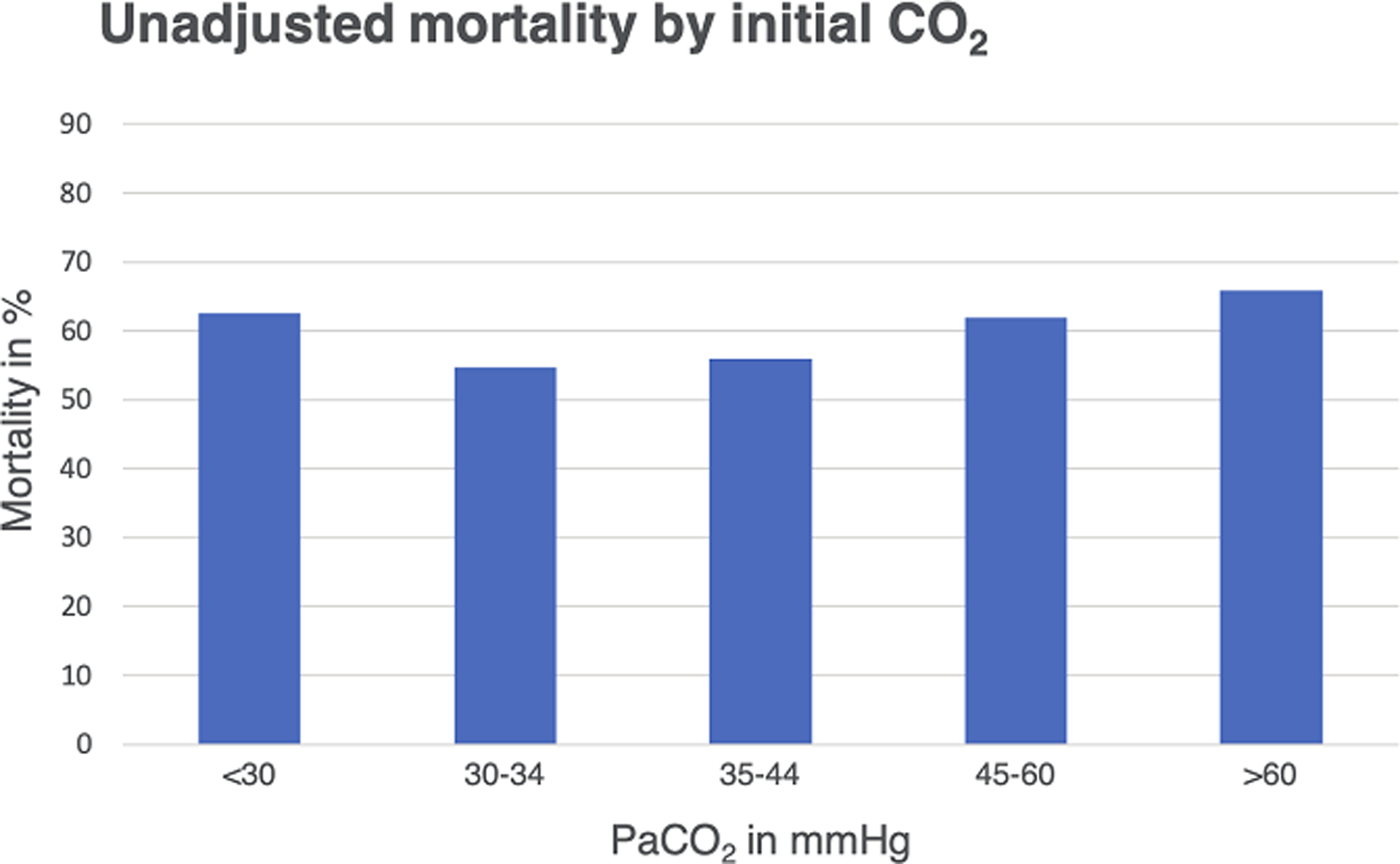
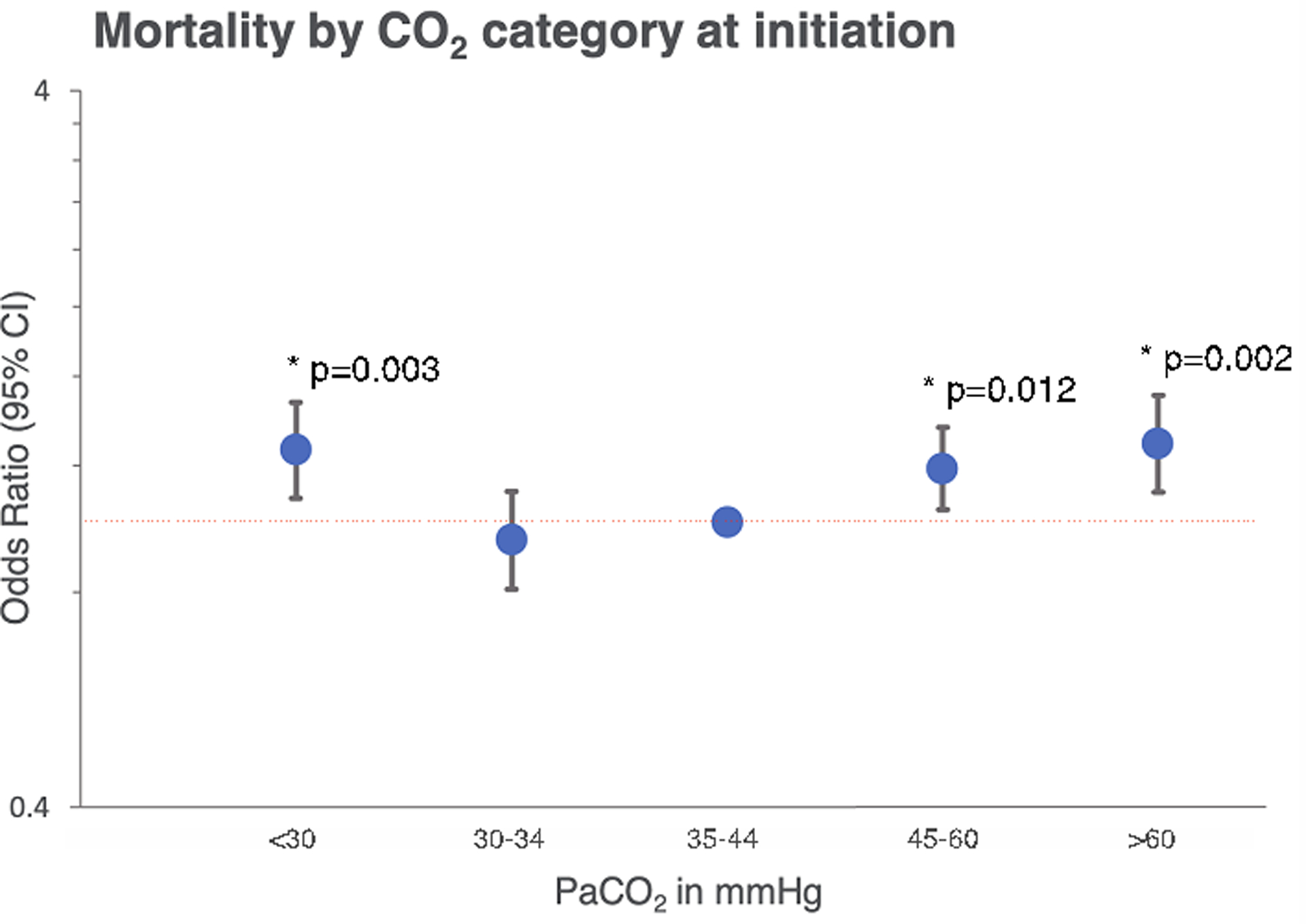
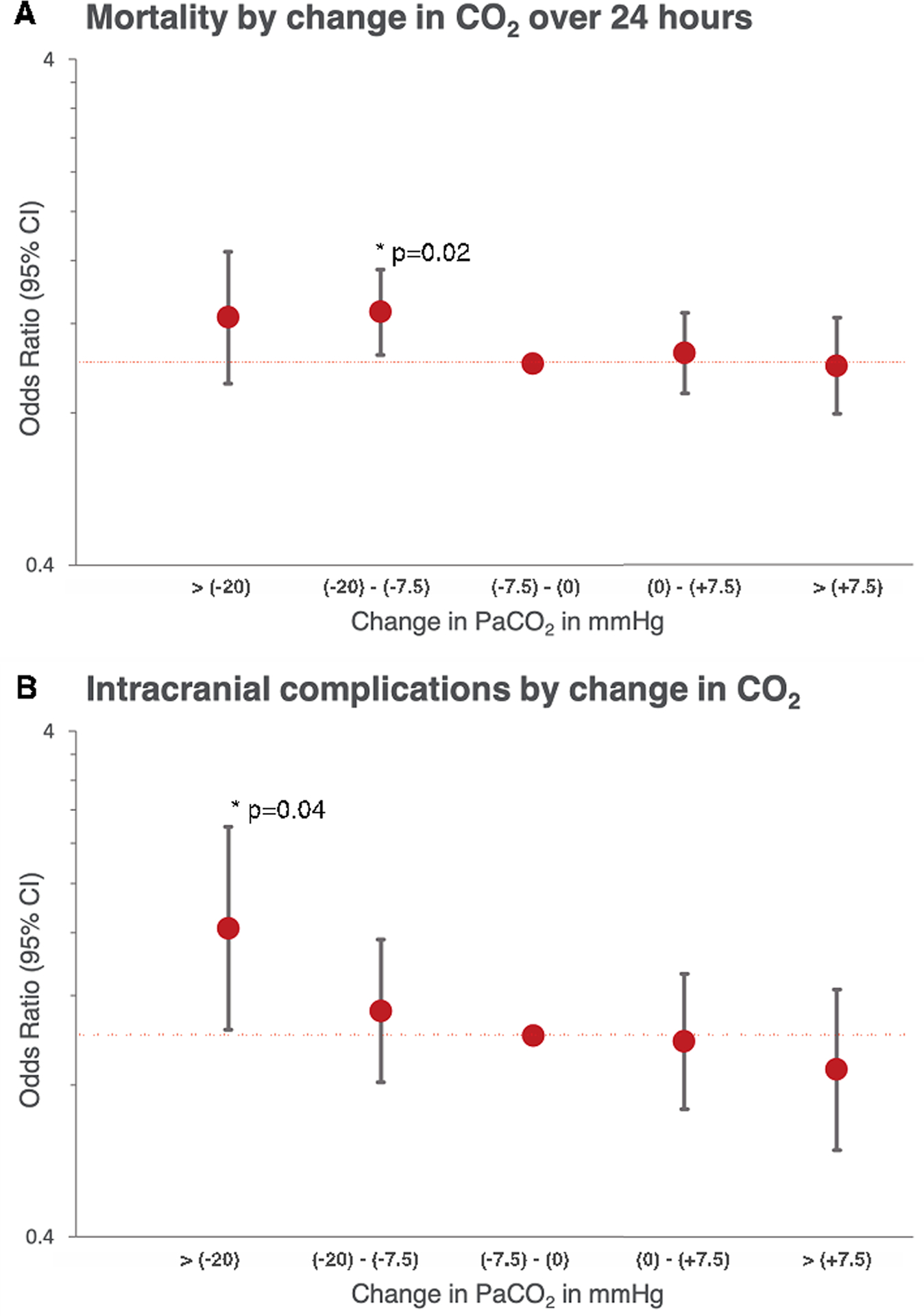
Measurements and main results: A total of 7,168 patients had sufficient data for analysis at the initiation of venoarterial extracorporeal membrane oxygenation, 4,918 of these patients had arterial carbon dioxide tension data available at 24 hours on support. The overall in-hospital mortality rate was 59.9%. A U-shaped relationship between arterial carbon dioxide tension tension at extracorporeal membrane oxygenation initiation and in-hospital mortality was observed. Increased mortality was observed with a arterial carbon dioxide tension less than 30 mm Hg (odds ratio, 1.26; 95% CI, 1.08-1.47; p = 0.003) and greater than 60 mm Hg (odds ratio, 1.28; 95% CI, 1.10-1.50; p = 0.002). Large reductions (> 20 mm Hg) in arterial carbon dioxide tension over 24 hours were associated with important neurologic complications: intracranial hemorrhage, ischemic stroke, and/or brain death, as a composite outcome (odds ratio, 1.63; 95% CI, 1.03-2.59; p = 0.04), independent of the initial arterial carbon dioxide tension.
Conclusions: Initial arterial carbon dioxide tension tension was independently associated with mortality in this cohort of venoarterial extracorporeal membrane oxygenation patients. Reductions in arterial carbon dioxide tension (> 20 mm Hg) from the initiation of extracorporeal membrane oxygenation were associated with neurologic complications. Further prospective studies testing these associations are warranted.
Figures
Comment in
-
Does the "Goldilocks Effect" Exist for Carbon Dioxide in Venoarterial Extracorporeal Membrane Oxygenation?Crit Care Med. 2020 Jul;48(7):1081-1082. doi: 10.1097/CCM.0000000000004361. Crit Care Med. 2020. PMID: 32568904 No abstract available.
-
The Effect of Changes of Arterial Carbon Dioxide Tension on Mortality May Differ Depending on the Initial Value.Crit Care Med. 2020 Dec;48(12):e1361-e1362. doi: 10.1097/CCM.0000000000004562. Crit Care Med. 2020. PMID: 33255126 No abstract available.
-
The authors reply.Crit Care Med. 2020 Dec;48(12):e1362. doi: 10.1097/CCM.0000000000004682. Crit Care Med. 2020. PMID: 33255127 No abstract available.
References
-
- Neumar RW, Nolan JP, Adrie C, et al. : Post-cardiac arrest syndrome: epidemiology, pathophysiology, treatment, and prognostication. A consensus statement from the International Liaison Committee on Resuscitation (American Heart Association, Australian and New Zealand Council on Resuscitation, European Resuscitation Council, Heart and Stroke Foundation of Canada, InterAmerican Heart Foundation, Resuscitation Council of Asia, and the Resuscitation Council of Southern Africa); the American Heart Association Emergency Cardiovascular Care Committee; the Council on Cardiovascular Surgery and Anesthesia; the Council on Cardiopulmonary, Perioperative, and Critical Care; the Council on Clinical Cardiology; and the Stroke Council. Circulation 2008; 118:2452–2483 - PubMed
-
- Marhong J, Fan E: Carbon dioxide in the critically ill: too much or too little of a good thing? Respir Care 2014; 59:1597–1605 - PubMed
-
- Carney N, Totten AM, O’Reilly C, et al. : Guidelines for the Management of Severe Traumatic Brain Injury, Fourth Edition. Neurosurgery 2017; 80:6–15 - PubMed
-
- Tiruvoipati R, Pilcher D, Buscher H, et al. : Effects of Hypercapnia and Hypercapnic Acidosis on Hospital Mortality in Mechanically Ventilated Patients. Crit Care Med 2017; 45:e649–e656 - PubMed
-
- Kregenow DA, Rubenfeld GD, Hudson LD, et al. : Hypercapnic acidosis and mortality in acute lung injury. Crit Care Med 2006; 34:1–7 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
