

The impact of increased chest compression fraction on survival for out-of-hospital cardiac arrest patients with a non-shockable initial rhythm
- PMID: 32574654
- PMCID: PMC7483839
- DOI: 10.1016/j.resuscitation.2020.06.016
The impact of increased chest compression fraction on survival for out-of-hospital cardiac arrest patients with a non-shockable initial rhythm
Abstract
Objective: We evaluated the effect of chest compression fraction (CCF) on survival to hospital discharge and return of spontaneous circulation (ROSC) in out-of-hospital cardiac arrest (OHCA) patients with non-shockable rhythms.
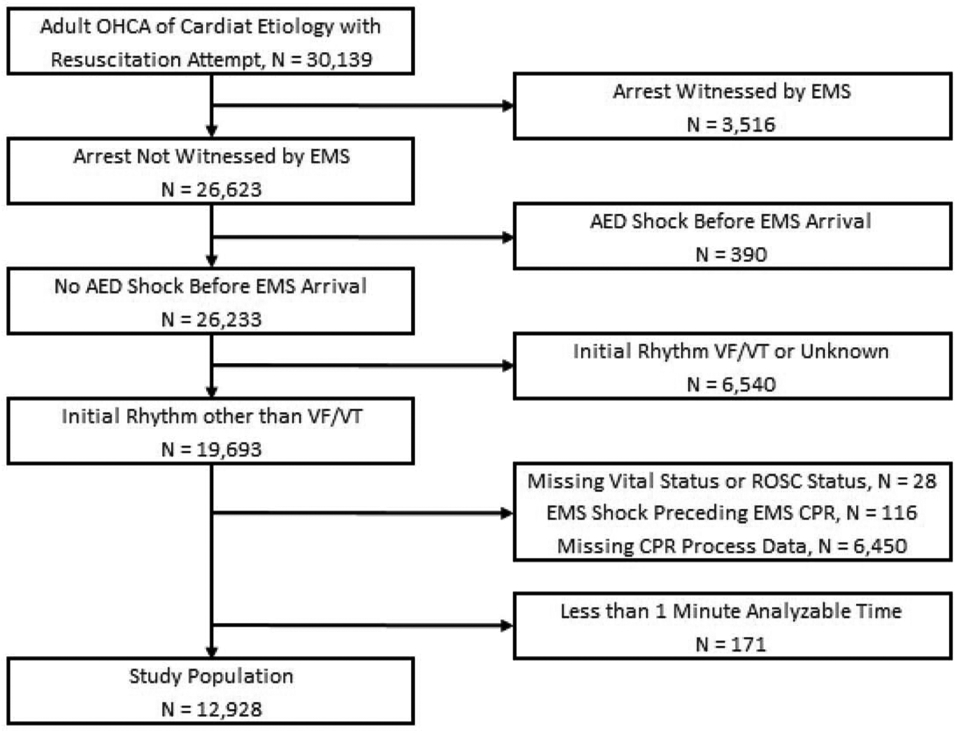
Methods: This is a retrospective analysis (completed in 2016) of a prospective cohort study which included OHCA patients from ten U.S. and Canadian sites (Resuscitation Outcomes Consortium Epistry and PRIMED study (2007-2011)). We included all OHCA victims of presumed cardiac aetiology, not witnessed by emergency medical services (EMS), without automated external defibrillator shock prior to EMS arrival, receiving > 1 min of CPR with CPR process measures available, and initial non-shockable rhythm. We measured CCF using the first 5 min of electronic CPR records.
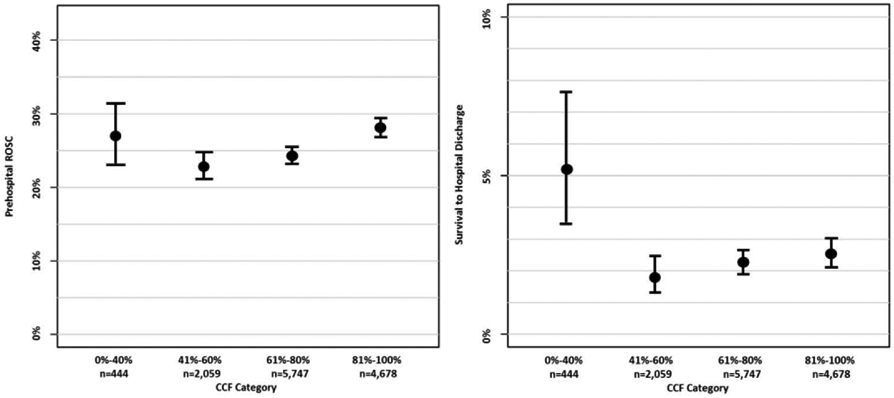
Results: Demographics of 12,928 adult patients were: mean age 68; male 59.9%; public location 8.5%; bystander witnessed 35.2%; bystander CPR 39.3%; median interval from 911 to defibrillator turned on 10 min:04 s; initial rhythm asystole 64.8%, PEA 26.0%, other non-shockable 9.2%; compression rate 80-120/min (69.1%); median CCF 74%; ROSC 25.6%; survival to hospital discharge 2.4%. Adjusted odds ratio (OR); 95% confidence intervals (95%CI) of survival for each CCF category were: 0-40% (2.00; 1.16, 3.32); 41-60% (0.83; 0.54, 1.24); 61-80% (1.02; 0.77, 1.35); and 81-100% (reference group). Adjusted (OR; 95%CI) of ROSC for each CCF category were: 0-40% (1.02; 0.79, 1.30); 41-60% (0.83; 0.72, 0.95); 61-80% (0.85; 0.77, 0.94); and 81-100% (reference group).
Conclusions: We observed an incremental benefit from higher CCF on the incidence of ROSC, but not survival, among non-shockable OHCA patients with CCF higher than 40%.
Keywords: Cardiopulmonary resuscitation; Heart arrest; Resuscitation.
Copyright © 2020 Elsevier B.V. All rights reserved.
Conflict of interest statement
CONFLICTS OF INTEREST
Dr. Cheskes has received investigator-initiated grant funding support and funding for educational speaking on CPR quality from Zoll Medical.
Dr. Nichol discloses salary support from University of Washington through Leonard A. Cobb Medic One Foundation Endowed Chair in Prehospital Emergency Care; Research support from ZOLL Medical Corp, Chelmsford, MA; Consultant to GE Healthcare Inc., Chicago, IL; Kestra Medical Technologies, Kirkland, WA; QOOL Therapeutics, Menlo Park, CA; and ZOLL Circulation Inc., San Jose, CA.
Figures
Comment in
-
What gaps in chest compressions tell us about gaps in CPR knowledge.Resuscitation. 2020 Sep;154:119-120. doi: 10.1016/j.resuscitation.2020.07.013. Epub 2020 Jul 22. Resuscitation. 2020. PMID: 32707145 No abstract available.
References
-
- Nichol G, Leroux B, Wang H, et al. Trial of Continuous or Interrupted Chest Compressions during CPR. New England Journal of Medicine. December 03 2015;373(23):2203–2214. - PubMed
-
- Vaillancourt C, Stiell IG, Canadian Cardiovascular Outcomes Research Team (CCORT). Cardiac arrest care and emergency medical services in Canada. Can J Cardiol. 2004;20(11):1081–1090. - PubMed
-
- Grunau B, Kawano T, Dick W, et al. Trends in care processes and survival following prehospital resuscitation improvement initiatives for out-of-hospital cardiac arrest in British Columbia, 2006-2016. Resuscitation. 2018;125:118–125. - PubMed
-
- Stiell IG, Wells GA, Field B, et al. Advanced cardiac life support in out-of-hospital cardiac arrest. New England Journal of Medicine. 2004;351(7):647–656. - PubMed
Publication types
MeSH terms
Grants and funding
- U01 HL077866/HL/NHLBI NIH HHS/United States
- U01 HL077871/HL/NHLBI NIH HHS/United States
- UL1 TR002494/TR/NCATS NIH HHS/United States
- U01 HL077865/HL/NHLBI NIH HHS/United States
- U01 HL077873/HL/NHLBI NIH HHS/United States
- U01 HL077881/HL/NHLBI NIH HHS/United States
- U01 HL077867/HL/NHLBI NIH HHS/United States
- U01 HL077872/HL/NHLBI NIH HHS/United States
- U01 HL077887/HL/NHLBI NIH HHS/United States
- U01 HL077885/HL/NHLBI NIH HHS/United States
- U01 HL077863/HL/NHLBI NIH HHS/United States
- U01 HL077908/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
