

A rare long-term undetected pheochromocytoma leading to Takotsubo syndrome in an older male patient: a case report
- PMID: 32576166
- PMCID: PMC7313138
- DOI: 10.1186/s12902-020-00578-5
A rare long-term undetected pheochromocytoma leading to Takotsubo syndrome in an older male patient: a case report
Abstract
Background: Takotsubo syndrome is an uncommon, acute, and reversible cardiomyopathy that occurs primarily in postmenopausal females. The clinical presentation of the syndrome resembles acute coronary syndrome, but coronary angiography reveals no obstructive coronary artery disease. Rarely, a catecholamine surge due to pheochromocytoma may induce Takotsubo syndrome. The clinical features of pheochromocytoma include paroxysmal hypertension, headache, palpitations, and profuse sweating. However, owing to the episodic, rather than continued, symptoms and signs of pheochromocytoma, its timely diagnosis poses a challenge for clinicians. Here, we report a rare case of long-term undetected pheochromocytoma leading to Takotsubo syndrome in an older male patient.
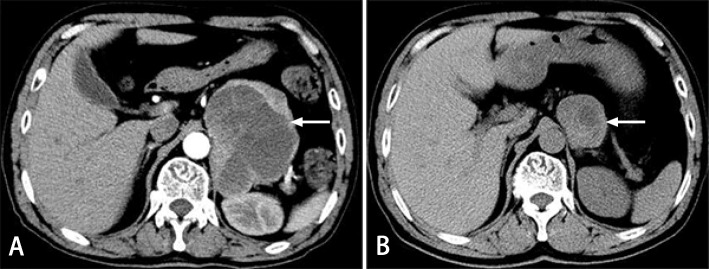
Case presentation: A 70-year-old man presented with paroxysmal chest distress and chest pain. Examinations revealed acute coronary syndrome with normal coronary arteries, heart failure, reversible left ventricular regional wall motion abnormalities, labile blood pressure, a giant left adrenal mass, and extremely high levels of metanephrine and normetanephrine. Clinical manifestations, laboratory reports, and imaging findings suggested a diagnosis of Takotsubo syndrome caused by pheochromocytoma. Supportive therapy, administration of alpha- adrenergic receptor blockers, and left adrenal mass resection resolved the patient's symptoms. A histological examination confirmed the presence of pheochromocytoma. We reviewed his history of midbrain hemorrhage 6 years prior and found a mass in the left adrenal region by reviewing the computed tomography images of the lung that were also taken 6 years prior, on which the pheochromocytoma was evident.
Conclusions: Our case illustrates the importance of understanding the link between pheochromocytoma and Takotsubo syndrome. A diagnosis of pheochromocytoma-induced Takotsubo syndrome should be considered during the differential diagnosis of acute coronary syndrome, especially in patients with labile blood pressure and normal coronary angiography findings; meanwhile, assessments of catecholamines and its metabolites and abdominal computed tomography scan should be performed at the right time. Clinicians should also be alert to potential pheochromocytoma in patients with unexplained cerebral hemorrhage, even in the absence of symptoms of catecholamine excess.
Keywords: Case report; Cerebral hemorrhage; Differential diagnosis; Pheochromocytoma; Takotsubo syndrome.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures


References
-
- Agarwal V, Kant G, Hans N, Messerli FH. Takotsubo-like cardiomyopathy in pheochromocytoma. Int J Cardiol. 2011;153(3):241–248. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
