

Efficacy and tolerability of the investigational topical cream SD-101 (6% allantoin) in patients with epidermolysis bullosa: a phase 3, randomized, double-blind, vehicle-controlled trial (ESSENCE study)
- PMID: 32576219
- PMCID: PMC7310548
- DOI: 10.1186/s13023-020-01419-3
Efficacy and tolerability of the investigational topical cream SD-101 (6% allantoin) in patients with epidermolysis bullosa: a phase 3, randomized, double-blind, vehicle-controlled trial (ESSENCE study)
Abstract
Background: Epidermolysis bullosa (EB) is a rare genetic disorder that manifests as blistering and/or skin erosion. There is no approved treatment for EB; current standard of care consists of wound and pain management. SD-101 6% is a topical cream containing 6% allantoin that was developed for treating skin lesions in patients with EB. The aim of this phase 3, multicenter, randomized, double-blind, vehicle-controlled study was to assess the efficacy and safety of SD-101 6% cream versus vehicle (0% allantoin) on lesions in patients with EB.
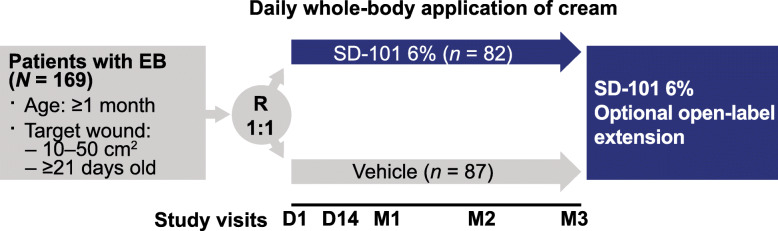
Methods: Eligible patients were ≥1 month old, had a diagnosis of EB (simplex, recessive dystrophic, or intermediate junctional) and a target wound 10-50 cm2 in size that was present for ≥21 days. Patients were randomly assigned to SD-101 6% cream or vehicle, which was applied topically once a day to the entire body for 3 months. Primary efficacy endpoints were time to complete target wound closure within 3 months and the proportion of patients who experienced complete target wound closure within 3 months. Post hoc subgroup analyses were conducted by patient age and in those with body surface area index of total body wound burden ≥5% at baseline.
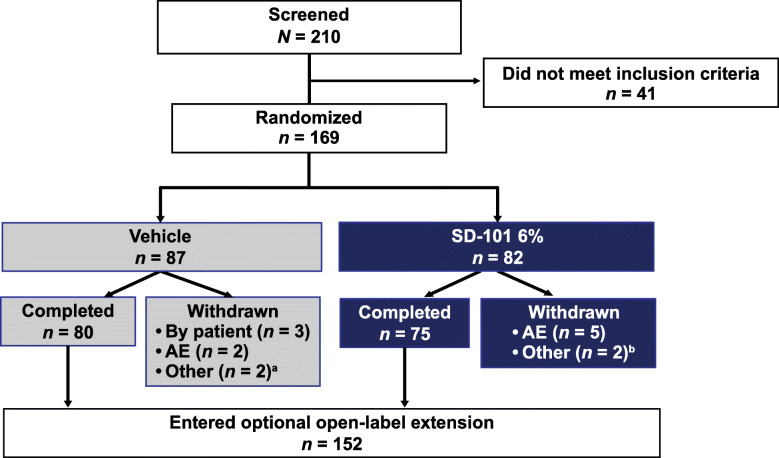
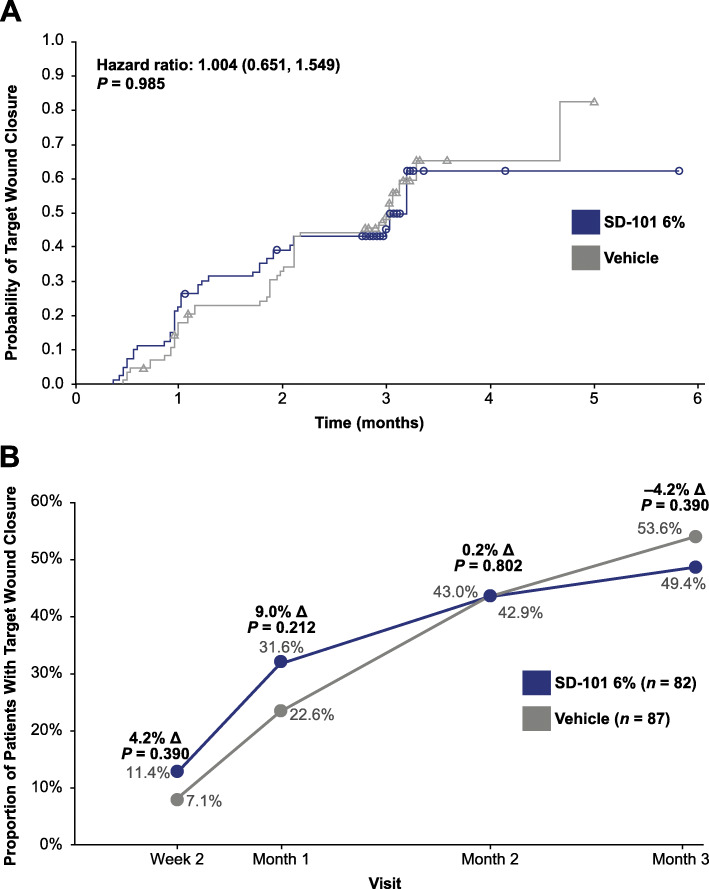
Results: In total, 169 patients were enrolled and randomly assigned to SD-101 6% (n = 82) or vehicle (n = 87). Baseline demographics and disease characteristics were similar between treatment groups. There were no statistically significant differences between treatment groups in time to target wound closure (hazard ratio, 1.004; 95% confidence interval [CI] 0.651, 1.549; P = 0.985) or proportion of patients with complete target wound closure within 3 months (odds ratio [95% CI], 0.733 [0.365, 1.474]; nominal P = 0.390). A positive trend toward faster wound closure with SD-101 6% versus vehicle was observed in patients aged 2 to <12 years and those with total body wound burden ≥5% at baseline. SD-101 6% cream was well tolerated.
Conclusions: SD-101 6% cream for treatment of EB-associated lesions was not more effective than vehicle in shortening the time to complete target wound closure or achieving complete target wound closure within 3 months.
Trial registration: ClinicalTrials.gov, NCT02384460; Date of trial registration, February 13, 2015; First participant enrolled, March 11, 2015.
Keywords: Allantoin; Efficacy; Epidermolysis bullosa; SD-101; Safety; Wound closure.
Conflict of interest statement
ASP has served as an investigator (uncompensated) for Amicus, Castle Creek Pharmaceuticals, Lenus Therapeutics, and Shire and as a consultant with honorarium for Castle Creek Pharmaceuticals, Lenus Therapeutics, and MEDACorp. JB has served as an investigator for Amicus, Galderma, Valeant, Patagonia, and Regeneron and as a speaker for Medimetriks and Promius. MN has received honoraria from Meda/Mylan, Medis, La Roche-Posay/L’Oreal, Uriage, Takeda, Novartis, Janssen, and Amicus. CB has served on advisory boards for Sanofi, as a consultant for Expanscience, as an investigator (uncompensated) for Amicus, as a speaker for La Roche-Posay and Expanscience, and has received honoraria from Celgene and Novartis. DFM has served as a consultant and investigator for Amicus, Amryt, Castle Creek Pharmaceuticals, and Shire and has conducted her own investigator-initiated randomized controlled trials in recessive dystrophic epidermolysis bullosa and epidermolysis bullosa simplex. EK is a paid consultant of Amicus. AR, HL, and JAB are employees of and hold stock in Amicus.
Figures
References
-
- Ma JE, Hand JL. What's new with common genetic skin disorders? Minerva Pediatr. 2017. - PubMed
-
- Brandling-Bennett HA, Morel KD. Common wound colonizers in patients with epidermolysis bullosa. Pediatr Dermatol. 2010;27(1):25–28. - PubMed
-
- Tabolli S, Pagliarello C, Uras C, Di Pietro C, Zambruno G, Castiglia D, et al. Family burden in epidermolysis bullosa is high independent of disease type/subtype. Acta Derm Venereol. 2010;90(6):607–611. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
