

The MD Anderson Prostate Cancer Patient-derived Xenograft Series (MDA PCa PDX) Captures the Molecular Landscape of Prostate Cancer and Facilitates Marker-driven Therapy Development
- PMID: 32576626
- PMCID: PMC7501166
- DOI: 10.1158/1078-0432.CCR-20-0479
The MD Anderson Prostate Cancer Patient-derived Xenograft Series (MDA PCa PDX) Captures the Molecular Landscape of Prostate Cancer and Facilitates Marker-driven Therapy Development
Abstract
Purpose: Advances in prostate cancer lag behind other tumor types partly due to the paucity of models reflecting key milestones in prostate cancer progression. Therefore, we develop clinically relevant prostate cancer models.
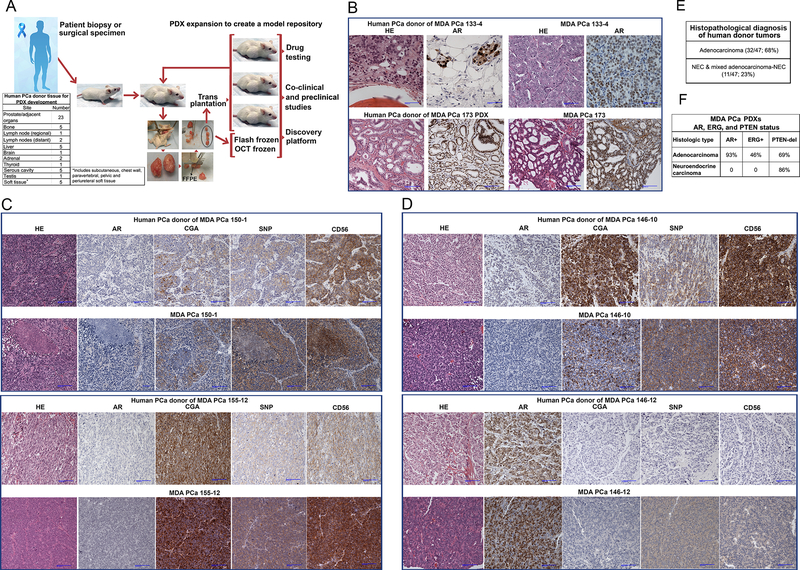
Experimental design: Since 1996, we have generated clinically annotated patient-derived xenografts (PDXs; the MDA PCa PDX series) linked to specific phenotypes reflecting all aspects of clinical prostate cancer.
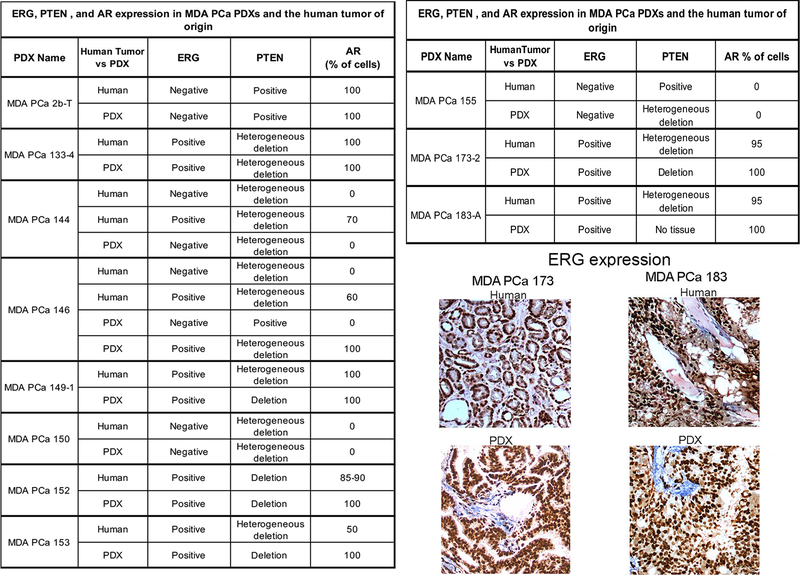
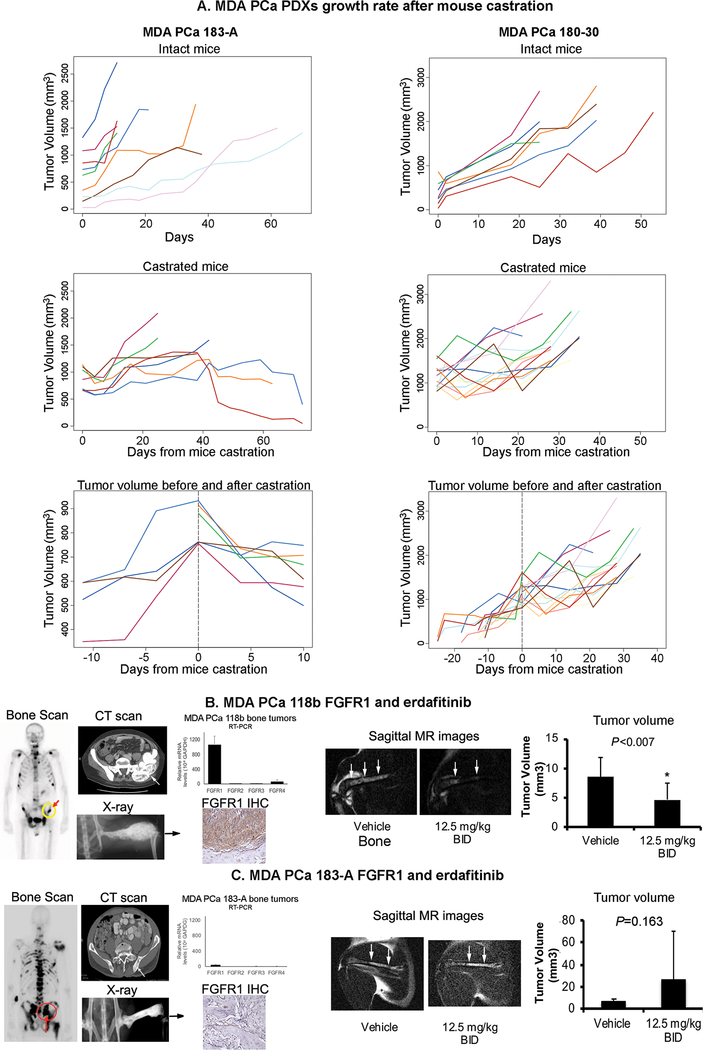
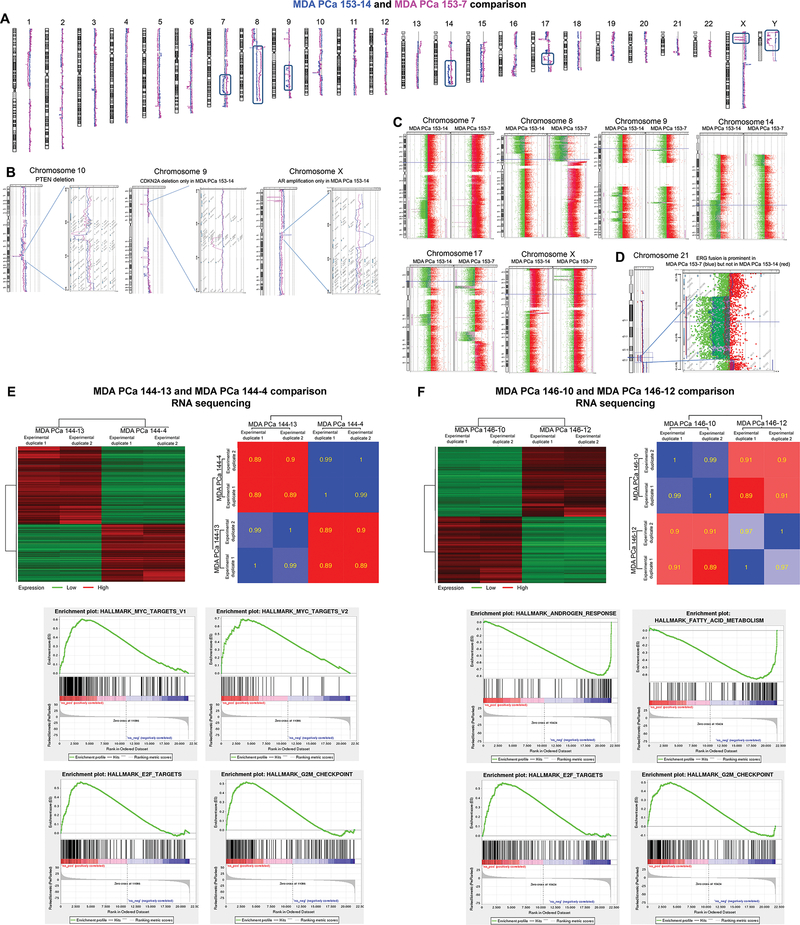
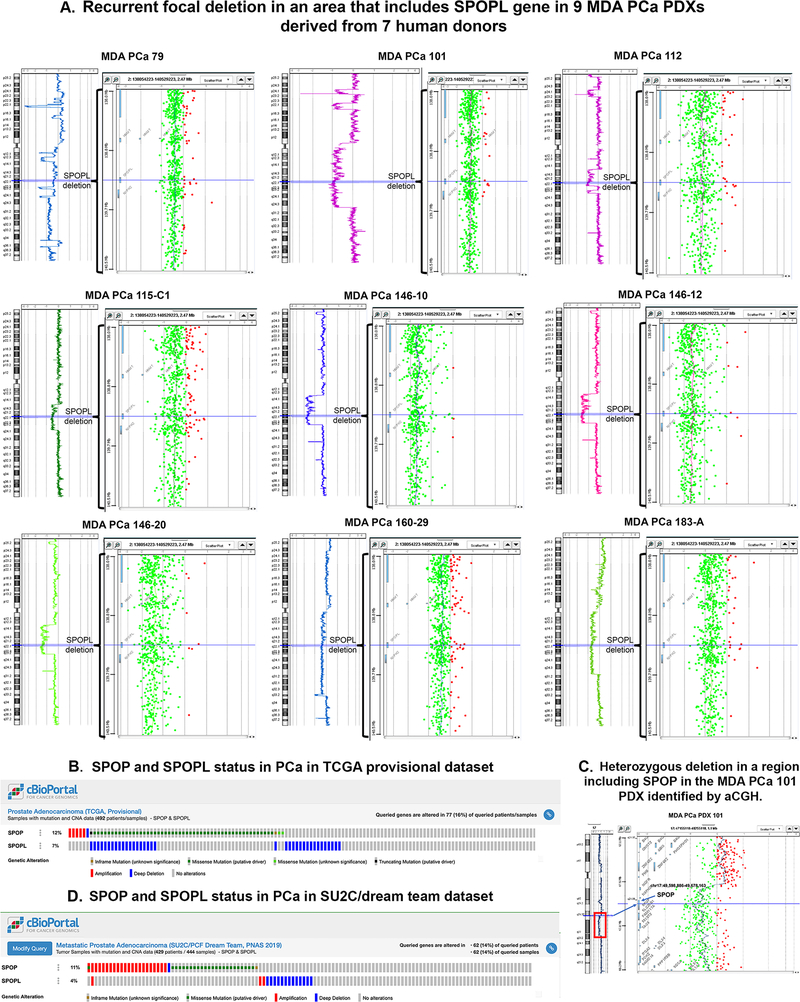
Results: We studied two cell line-derived xenografts and the first 80 PDXs derived from 47 human prostate cancer donors. Of these, 47 PDXs derived from 22 donors are working models and can be expanded either as cell lines (MDA PCa 2a and 2b) or PDXs. The histopathologic, genomic, and molecular characteristics (androgen receptor, ERG, and PTEN loss) maintain fidelity with the human tumor and correlate with published findings. PDX growth response to mouse castration and targeted therapy illustrate their clinical utility. Comparative genomic hybridization and sequencing show significant differences in oncogenic pathways in pairs of PDXs derived from different areas of the same tumor. We also identified a recurrent focal deletion in an area that includes the speckle-type POZ protein-like (SPOPL) gene in PDXs derived from seven human donors of 28 studied (25%). SPOPL is a SPOP paralog, and SPOP mutations define a molecular subclass of prostate cancer. SPOPL deletions are found in 7% of The Cancer Genome Atlas prostate cancers, which suggests that our cohort is a reliable platform for targeted drug development.
Conclusions: The MDA PCa PDX series is a dynamic resource that captures the molecular landscape of prostate cancers progressing under novel treatments and enables optimization of prostate cancer-specific, marker-driven therapy.
©2020 American Association for Cancer Research.
Conflict of interest statement
Figures
Similar articles
-
Patient-Derived Xenograft Models for Translational Prostate Cancer Research and Drug Development.Methods Mol Biol. 2024;2806:153-185. doi: 10.1007/978-1-0716-3858-3_12. Methods Mol Biol. 2024. PMID: 38676802
-
Integrative Molecular Analyses of the MD Anderson Prostate Cancer Patient-derived Xenograft (MDA PCa PDX) Series.Clin Cancer Res. 2024 May 15;30(10):2272-2285. doi: 10.1158/1078-0432.CCR-23-2438. Clin Cancer Res. 2024. PMID: 38488813 Free PMC article.
-
Movember GAP1 PDX project: An international collection of serially transplantable prostate cancer patient-derived xenograft (PDX) models.Prostate. 2018 Dec;78(16):1262-1282. doi: 10.1002/pros.23701. Epub 2018 Aug 2. Prostate. 2018. PMID: 30073676
-
Application of Prostate Cancer Models for Preclinical Study: Advantages and Limitations of Cell Lines, Patient-Derived Xenografts, and Three-Dimensional Culture of Patient-Derived Cells.Cells. 2019 Jan 20;8(1):74. doi: 10.3390/cells8010074. Cells. 2019. PMID: 30669516 Free PMC article. Review.
-
Patient derived organoids in prostate cancer: improving therapeutic efficacy in precision medicine.Mol Cancer. 2021 Sep 29;20(1):125. doi: 10.1186/s12943-021-01426-3. Mol Cancer. 2021. PMID: 34587953 Free PMC article. Review.
Cited by
-
Experimental in vitro, ex vivo and in vivo models in prostate cancer research.Nat Rev Urol. 2023 Mar;20(3):158-178. doi: 10.1038/s41585-022-00677-z. Epub 2022 Nov 30. Nat Rev Urol. 2023. PMID: 36451039 Review.
-
Targeting IL-8 and Its Receptors in Prostate Cancer: Inflammation, Stress Response, and Treatment Resistance.Cancers (Basel). 2024 Aug 8;16(16):2797. doi: 10.3390/cancers16162797. Cancers (Basel). 2024. PMID: 39199570 Free PMC article. Review.
-
New mouse models for exploring renal tumor extension into the inferior vena cava.Commun Biol. 2025 Mar 5;8(1):359. doi: 10.1038/s42003-025-07757-x. Commun Biol. 2025. PMID: 40044768 Free PMC article.
-
Unraveling the Global Proteome and Phosphoproteome of Prostate Cancer Patient-Derived Xenografts.Mol Cancer Res. 2024 May 2;22(5):452-464. doi: 10.1158/1541-7786.MCR-23-0976. Mol Cancer Res. 2024. PMID: 38345532 Free PMC article.
-
Targeting the lipid kinase PIKfyve upregulates surface expression of MHC class I to augment cancer immunotherapy.Proc Natl Acad Sci U S A. 2023 Dec 5;120(49):e2314416120. doi: 10.1073/pnas.2314416120. Epub 2023 Nov 27. Proc Natl Acad Sci U S A. 2023. PMID: 38011559 Free PMC article.
References
-
- Navone NM, van Weerden WM, Vessella RL, Williams ED, Wang Y, Isaacs JT, et al. Movember GAP1 PDX project: An international collection of serially transplantable prostate cancer patient-derived xenograft (PDX) models. Prostate. 2018;78(16):1262–82. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
