

Unusual iodine-131 postablation whole-body scintigraphy patterns in patients after robot-assisted/endoscopic thyroidectomy: Case series
- PMID: 32577243
- PMCID: PMC7303882
- DOI: 10.1002/ccr3.2795
Unusual iodine-131 postablation whole-body scintigraphy patterns in patients after robot-assisted/endoscopic thyroidectomy: Case series
Abstract
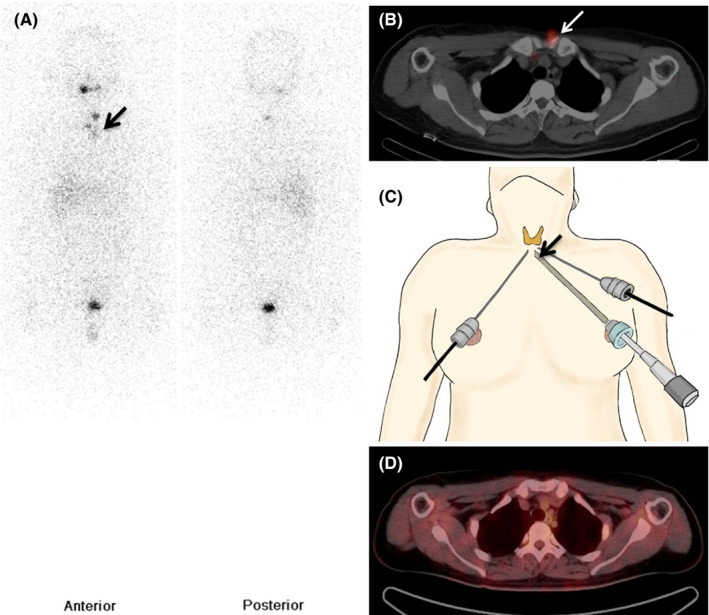
Robot-assisted/endoscopic thyroidectomy causes irritation due to instruments or implantation of thyroid tissue on the anterior chest wall and lower neck. We present three patients who exhibited unexpected focal lesions on postablation Iodine-131 single-photon emission computed tomography/computed tomography without biochemical and structural diseases. Meticulous surgical techniques are important to prevent complications.
Keywords: Iodine‐131 whole‐body scintigraphy (WBS); endoscopic thyroidectomy; positron emission tomography/computed tomography (PET/CT); robot‐assisted thyroidectomy; single‐photon emission computed tomography/computed tomography (SPECT/CT); thyroid carcinoma; unusual patterns.
© 2020 The Authors. Clinical Case Reports published by John Wiley & Sons Ltd.
Conflict of interest statement
The authors declare that there are no conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures


References
-
- Lee KE, Kim HY, Park WS, et al. Postauricular and axillary approach endoscopic neck surgery: a new technique. World J Surg. 2009;33(4):767‐772. - PubMed
-
- Ikeda Y, Takami H, Tajima G, et al. Total endoscopic thyroidectomy: axillary or anterior chest approach. Biomed Pharmacother. 2002;56(Suppl 1):72s‐78s. - PubMed
-
- Jung CH, Kim BY, Kim JW, et al. False‐positive F‐18 FDG PET/CT from foreign body reaction on anterior chest wall after endoscopic total thyroidectomy via axillo‐breast approach for thyroid cancer: two case reports. Clin Nucl Med. 2011;36(11):1036‐1038. - PubMed
-
- Kim HR, Hong HS, Lee EH, et al. Ultrasonographic findings of foreign‐body granulomas after endoscopic thyroidectomy via an axillo‐breast approach. J Korean Soc Radiol. 2012;66(6):507‐517.
Publication types
LinkOut - more resources
Full Text Sources
