

Complete revascularization for patients with multivessel coronary artery disease and ST-segment elevation myocardial infarction after the COMPLETE trial: A meta-analysis of randomized controlled trials
- PMID: 32577495
- PMCID: PMC7301199
- DOI: 10.1016/j.ijcha.2020.100549
Complete revascularization for patients with multivessel coronary artery disease and ST-segment elevation myocardial infarction after the COMPLETE trial: A meta-analysis of randomized controlled trials
Erratum in
-
Erratum regarding missing Declaration of Competing Interest statements in previously published articles.Int J Cardiol Heart Vasc. 2020 Dec 19;32:100699. doi: 10.1016/j.ijcha.2020.100699. eCollection 2021 Feb. Int J Cardiol Heart Vasc. 2020. PMID: 33681452 Free PMC article.
Abstract
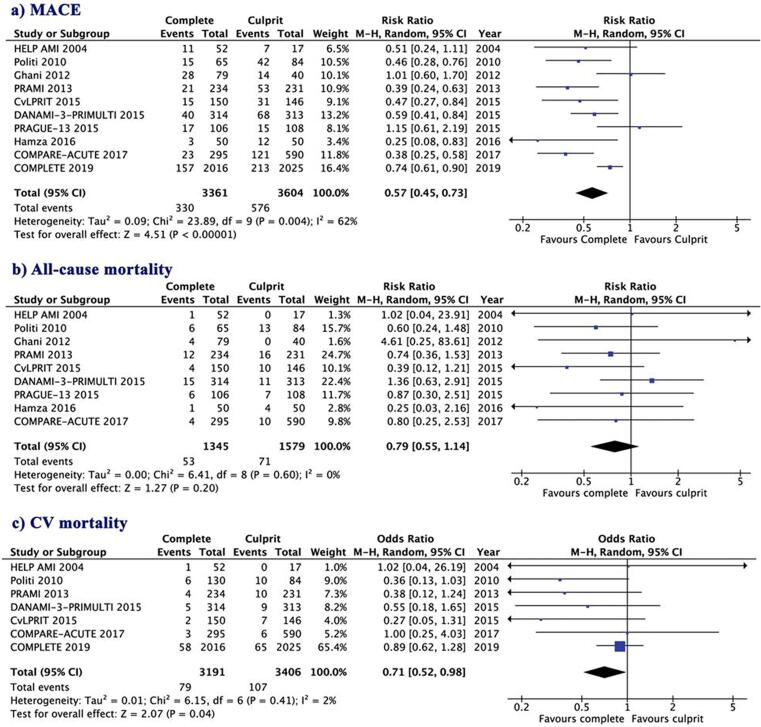
Background: The recently published COMPLETE trial has demonstrated that patients with ST-segment elevation myocardial infarction (STEMI) and multivessel coronary artery disease (MVD), who underwent successful percutaneous coronary intervention (PCI) of both culprit and non-culprit (vs. culprit-only) lesions had a reduced risk of major adverse cardiac events (MACE), but not of cardiovascular or total mortality. The aim of this meta-analysis was to assess the efficacy of complete revascularization on cardiovascular or total mortality reduction using available randomized controlled trials (RCTs) including the COMPLETE trial, in hemodynamically stable STEMI patients with MVD.
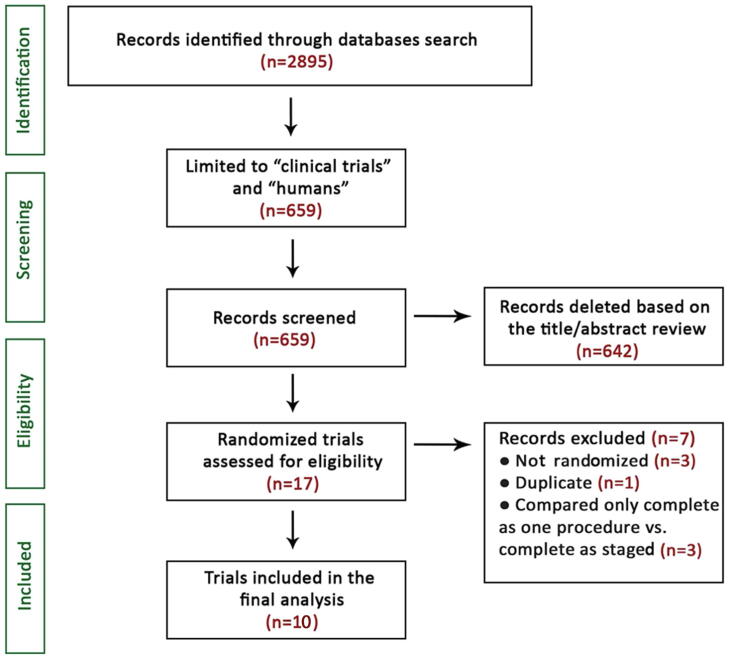
Methods: PubMed, MEDLINE, Embase, Scopus, Google Scholar, CENTRAL and ClinicalTrials.gov databases search identified 10 RCTs of 7033 patients with STEMI and MVD which compared complete (n = 3420) vs. only culprit lesion (n = 3613) PCI for a median 27.7 months follow-up. Random effect risk ratios were used to estimate for efficacy and safety outcomes.
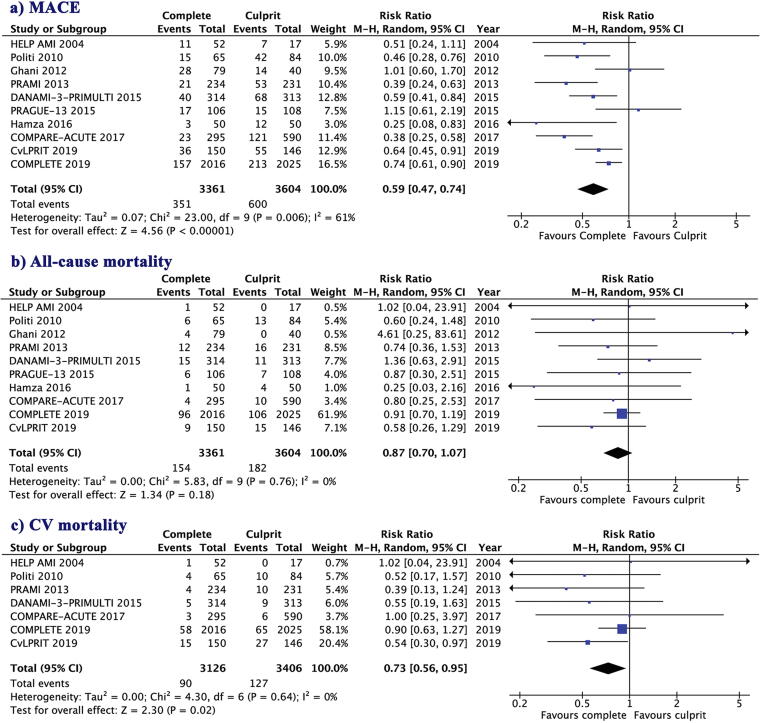
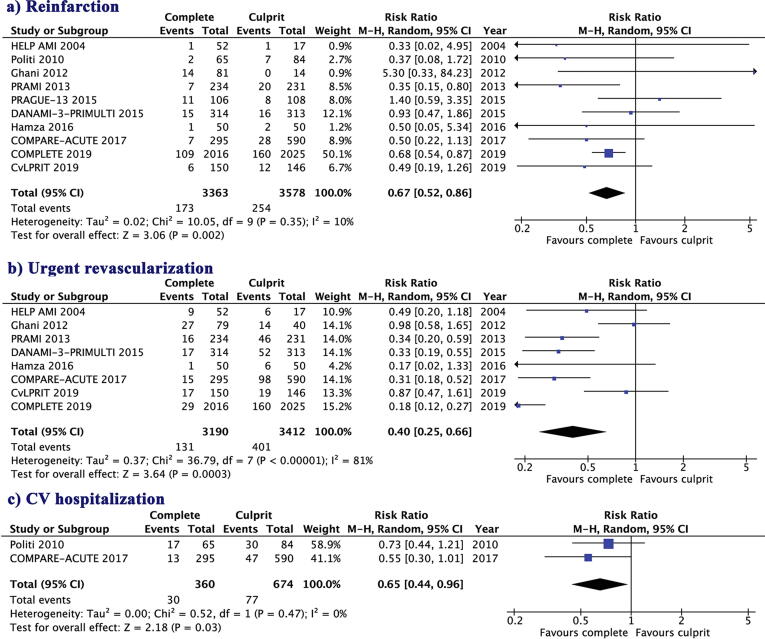
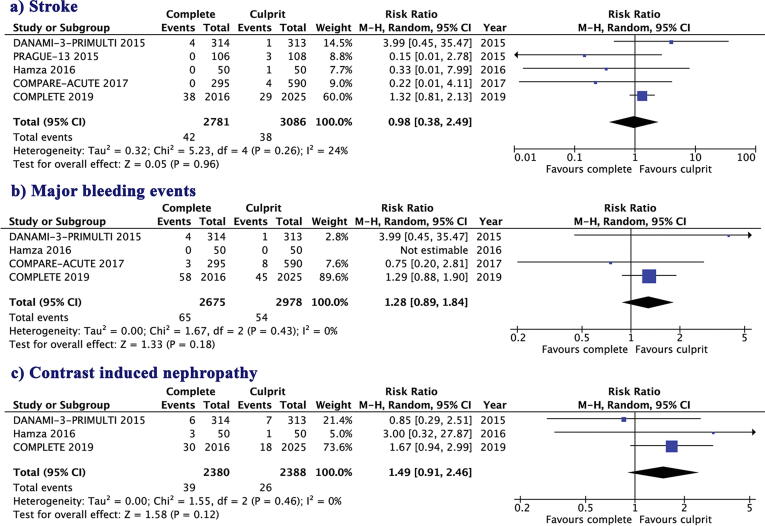
Results: Complete revascularization reduced the risk of MACE (10.4% vs.16.6%; RR = 0.59, 95% CI: 0.47 to 0.74, p < 0.0001), CV mortality (2.87% vs. 3.72%; RR = 0.73, 95% CI: 0.56 to 0.95, p = 0.02), reinfarction (5.1% vs. 7.1%; RR = 0.67, 95% CI: 0.52 to 0.86, p = 0.002), urgent revascularization (7.92% vs.17.4%; RR = 0.47, 95% CI: 0.30 to 0.73, p < 0.001), and CV hospitalization (8.68% vs.11.4%; RR = 0.65, 95% CI: 0.44to 0.96, p = 0.03) compared with culprit only revascularization. All-cause mortality, stroke, major bleeding events, or contrast induced nephropathy were not affected by the revascularization strategy.
Conclusion: The findings of this meta-analysis suggest that in patients with STEMI and MVD, complete revascularization is superior to culprit-only PCI in reducing the risk of MACE outcomes, including cardiovascular mortality, without increasing the risk of adverse safety outcomes.
Keywords: Complete revascularization; Coronary artery disease; Infarct artery only revascularization; Multi-vessel disease; ST-segment elevation myocardial infarction.
© 2020 The Authors. Published by Elsevier B.V.
Figures
References
-
- Keeley E.C., Boura J.A., Grines C.L. Primary angioplasty versus intravenous thrombolytic therapy for acute myocardial infarction: a quantitative review of 23 randomised trials. Lancet. 2003;361(9351):13–20. - PubMed
-
- Ibanez B., James S., Agewall S., Antunes M.J., Bucciarelli-Ducci C., Bueno H. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: The Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC) Eur. Heart J. 2018;39(2):119–177. - PubMed
-
- Wong G.C., Welsford M., Ainsworth C., Abuzeid W., Fordyce C.B., Greene J. 2019 Canadian Cardiovascular Society/Canadian Association of Interventional Cardiology Guidelines on the Acute Management of ST-Elevation Myocardial Infarction: Focused Update on Regionalization and Reperfusion. Can. J. Cardiol. 2019;35(2):107–132. - PubMed
-
- Cardarelli F., Bellasi A., Ou F.S., Shaw L.J., Veledar E., Roe M.T. Combined impact of age and estimated glomerular filtration rate on in-hospital mortality after percutaneous coronary intervention for acute myocardial infarction (from the American College of Cardiology National Cardiovascular Data Registry) Am. J. Cardiol. 2009;103(6):766–771. - PubMed
-
- Sorajja P., Gersh B.J., Cox D.A., McLaughlin M.G., Zimetbaum P., Costantini C. Impact of multivessel disease on reperfusion success and clinical outcomes in patients undergoing primary percutaneous coronary intervention for acute myocardial infarction. Eur. Heart J. 2007;28(14):1709–1716. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
