

This is a preprint.
Longitudinal Surveillance for SARS-CoV-2 Among Staff in Six Colorado Long-Term Care Facilities: Epidemiologic, Virologic and Sequence Analysis
- PMID: 32577700
- PMCID: PMC7302309
- DOI: 10.1101/2020.06.08.20125989
Longitudinal Surveillance for SARS-CoV-2 Among Staff in Six Colorado Long-Term Care Facilities: Epidemiologic, Virologic and Sequence Analysis
Update in
-
Early Adoption of Longitudinal Surveillance for SARS-CoV-2 among Staff in Long-Term Care Facilities: Prevalence, Virologic and Sequence Analysis.Microbiol Spectr. 2021 Dec 22;9(3):e0100321. doi: 10.1128/Spectrum.01003-21. Epub 2021 Nov 10. Microbiol Spectr. 2021. PMID: 34756092 Free PMC article.
Abstract
Background: SARS-CoV-2 emerged in 2019 and has become a major global pathogen. Its emergence is notable due to its impacts on individuals residing within long term care facilities (LTCFs) such as rehabilitation centers and nursing homes. LTCF residents tend to possess several risk factors for more severe SARS-CoV-2 outcomes, including advanced age and multiple comorbidities. Indeed, residents of LTCFs represent approximately 40% of SARS-CoV-2 deaths in the United States.
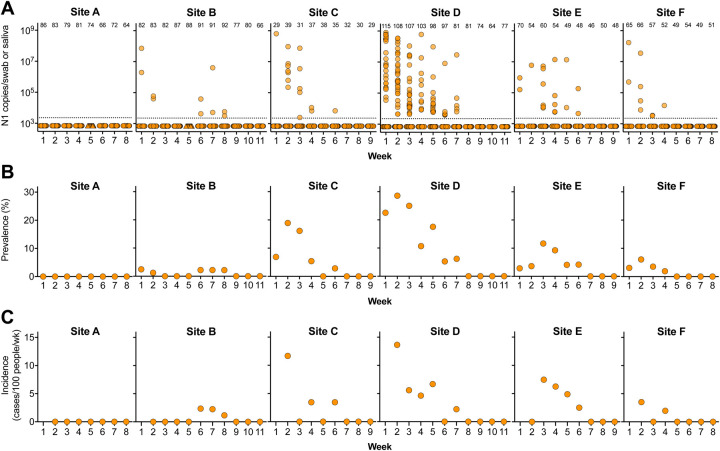
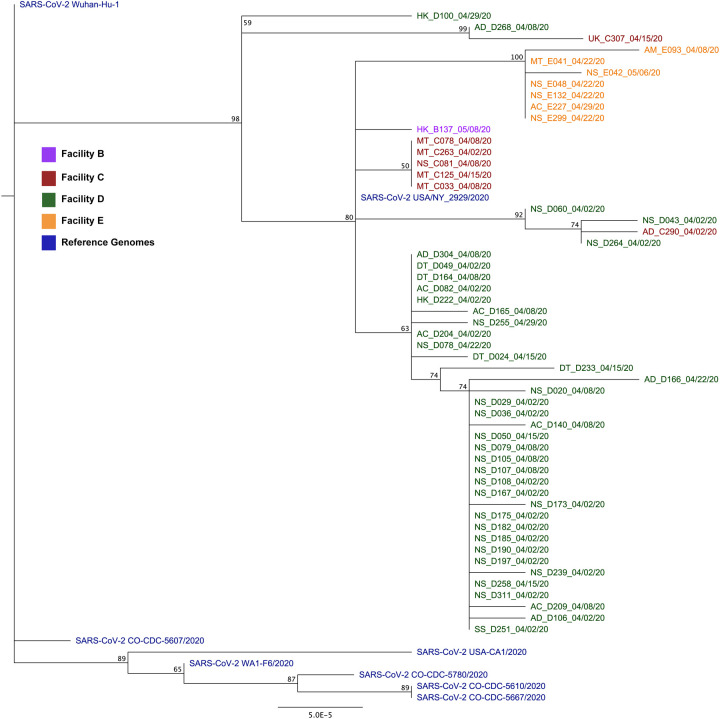
Methods: To assess the prevalence and incidence of SARS-CoV-2 among LTCF workers, determine the extent of asymptomatic SARS-CoV-2 infection, and provide information on the genomic epidemiology of the virus within these unique care settings, we collected nasopharyngeal swabs from workers for 8-11 weeks at six Colorado LTCFs, determined the presence and level of viral RNA and infectious virus within these samples, and sequenced 54 nearly complete genomes.
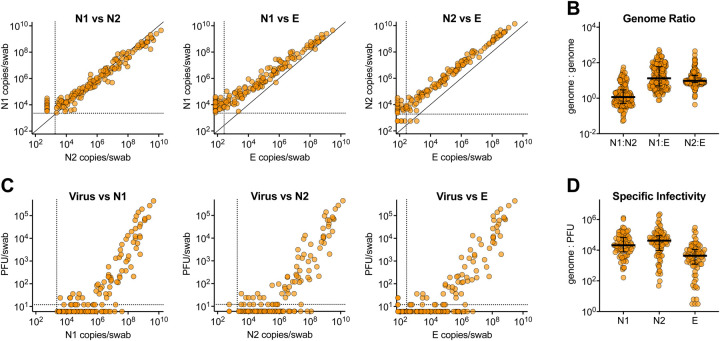
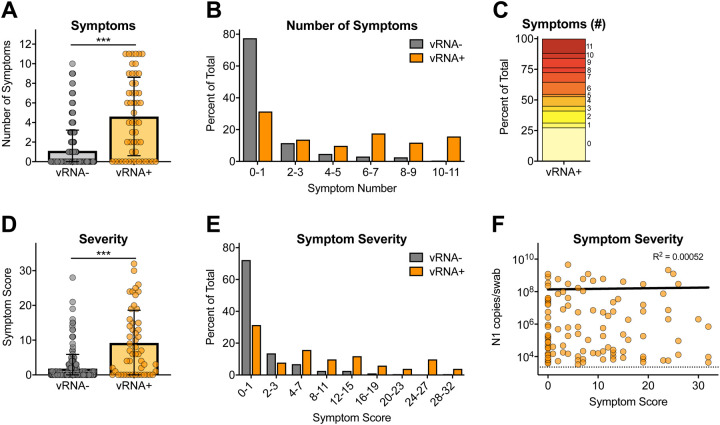
Findings: Our data reveal a strikingly high degree of asymptomatic/mildly symptomatic infection, a strong correlation between viral RNA and infectious virus, prolonged infections and persistent RNA in a subset of individuals, and declining incidence over time.
Interpretation: Our data suggest that asymptomatic SARS-CoV-2 infected individuals contribute to virus persistence and transmission within the workplace, due to high levels of virus. Genetic epidemiology revealed that SARS-CoV-2 likely spreads between staff within an LTCF.
Funding: Colorado State University Colleges of Health and Human Sciences, Veterinary Medicine and Biomedical Sciences, Natural Sciences, and Walter Scott, Jr. College of Engineering, the Columbine Health Systems Center for Healthy Aging, and the National Institute of Allergy and Infectious Diseases.
Figures

References
-
- CDC. Preparing for COVID-19 in Nursing Homes. 2020; Available from: https://www.cdc.gov/coronavirus/2019-ncov/hcp/long-term-care.html.
-
- The Nursing Home COVID-19 Public File. 2020; Available from: https://data.cms.gov/stories/s/COVID-19-Nursing-Home-Data/bkwz-xpvg/.
-
- More Than 40% of U.S. Coronavirus Deaths Are Linked to Nursing Homes. 2020; Available from: https://www.nytimes.com/interactive/2020/us/coronavirus-nursing-homes.html.
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous