

Healthy Lifestyle for Prevention of Premature Death Among Users and Nonusers of Common Preventive Medications: A Prospective Study in 2 US Cohorts
- PMID: 32578485
- PMCID: PMC7670542
- DOI: 10.1161/JAHA.119.016692
Healthy Lifestyle for Prevention of Premature Death Among Users and Nonusers of Common Preventive Medications: A Prospective Study in 2 US Cohorts
Abstract
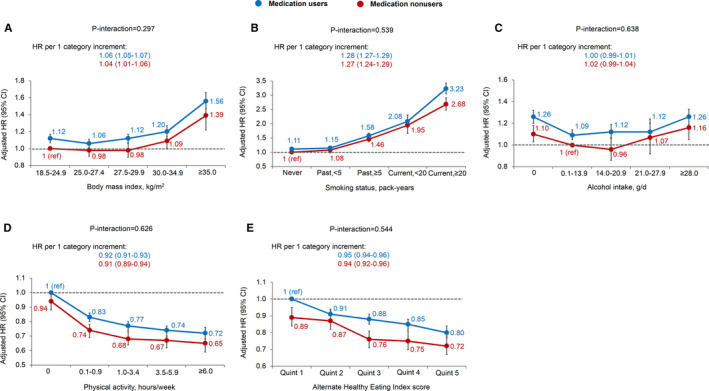
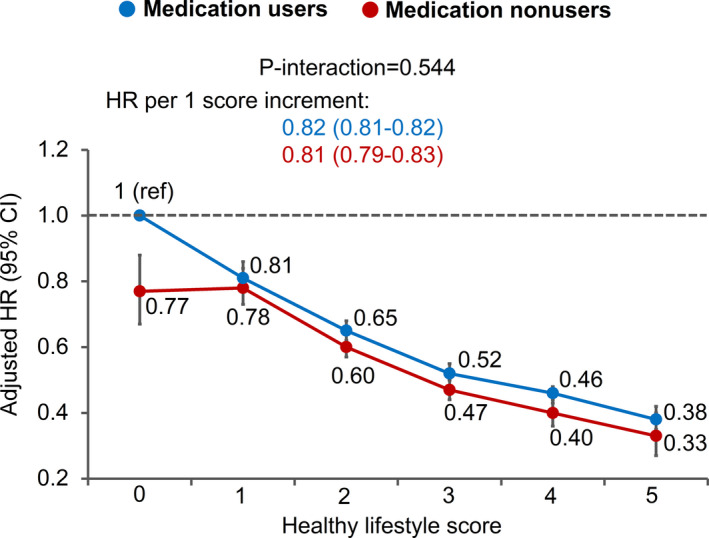
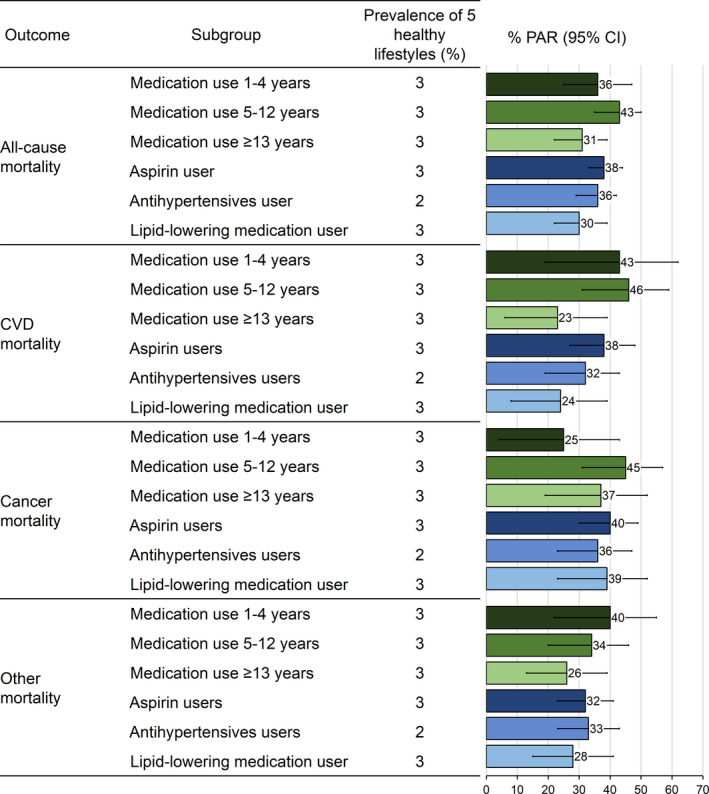
Background It remains unknown whether individuals who regularly use preventive medications receive the same benefit from healthy lifestyle as those who do not use medications. We aimed to examine the associations of healthy lifestyle with mortality according to use of major preventive medications, including aspirin, antihypertensives, and lipid-lowering medications. Methods and Results Among 79 043 women in the Nurses' Health Study (1988-2014) and 39 544 men in the Health Professionals Follow-up Study (1986-2014), we defined a healthy lifestyle score based on body mass index, smoking, physical activity, diet, and alcohol intake. We estimated multivariable hazard ratios (HRs) and population-attributable risks of death from any cause, cardiovascular disease, cancer, and other causes in relation to healthy lifestyle according to medication use. We documented 35 195 deaths. A similar association of healthy lifestyle score with lower all-cause mortality was observed among medication users (HR, 0.82 per unit increment; 95% CI, 0.81-0.82) and nonusers (HR, 0.81; 95% CI, 0.79-0.83) (P interaction=0.54). The fraction of premature deaths that might be prevented by adherence to the 5 healthy lifestyle factors among medication users and nonusers was 38% (95% CI, 32%-42%) and 40% (95% CI, 29%-50%) for all-cause mortality, 37% (95% CI, 27%-46%) and 45% (95% CI, 18%-66%) for cardiovascular disease mortality, and 38% (95% CI, 28%-46%) and 33% (95% CI, 14%-49%) for cancer mortality, respectively. Conclusions Adherence to a healthy lifestyle confers substantial benefit for prevention of premature death among both regular users and nonusers of preventive medications. Adherence to a healthy lifestyle remains important even among individuals regularly using preventive medications.
Keywords: lifestyle; mortality; nutrition; preventive medication; primary prevention.
Conflict of interest statement
Our study has several strengths, including the large sample size, long‐term follow‐up of up to 28 years, detailed and repeated assessment of medication use, and rigorous adjustment for potential confounding factors. Several limitations should also be noted. First, we applied a less stringent threshold to define healthy lifestyle (eg, the upper limit for BMI was set at 27.5 rather than 25, as commonly used to define normal body weight) to preserve statistical power because even with the current threshold, only 3% to 4% of participants met the healthy criteria for all of the 5 lifestyle factors. Therefore, the PARs for healthy lifestyles may have been underestimated. Second, our medication, lifestyle, and anthropometric (eg, height and weight) data were all based on self‐report and thus subject to measurement error. However, the accuracy and stability of these self‐reported data have been well documented in our cohorts, 52 , 53 , 54 as well as other study populations. 55 Third, our study participants were all health professionals and predominantly white, thereby limiting our ability to stratify the analyses by race and reducing the generalizability of our findings. However, it is unlikely that the biological effect of lifestyle would have a substantial difference between health professionals and the general population. Moreover, given the higher health consciousness and better lifestyle profiles of health professionals, we may have underestimated the benefit of lifestyles on the population scale.
A healthy lifestyle may confer similar substantial benefit in preventing premature death in regular users and nonusers of preventive medications. Adherence to a healthy lifestyle is still important even among individuals regularly using preventive medications.
Chan previously served as a consultant for Bayer Healthcare and Pfizer Inc. for work unrelated to the topic of this article. This study was not funded by Bayer Healthcare or Pfizer Inc. The remaining authors have no disclosures to report.
Figures
References
-
- Murphy SL, Xu J, Kochanek KD, Arias E. Mortality in the United States, 2017. NCHS Data Brief. 2018;1–8. - PubMed
-
- Williams CD, Chan AT, Elman MR, Kristensen AH, Miser WF, Pignone MP, Stafford RS, McGregor JC. Aspirin use among adults in the U.S.: results of a national survey. Am J Prev Med. 2015;501–508. - PubMed
-
- Gu Q, Paulose‐Ram R, Burt VL, Kit BK. Prescription cholesterol‐lowering medication use in adults aged 40 and over: United States, 2003–2012. NCHS Data Brief. 2014;1–8. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
