

Heating technology for malignant tumors: a review
- PMID: 32579419
- PMCID: PMC7781160
- DOI: 10.1080/02656736.2020.1779357
Heating technology for malignant tumors: a review
Abstract
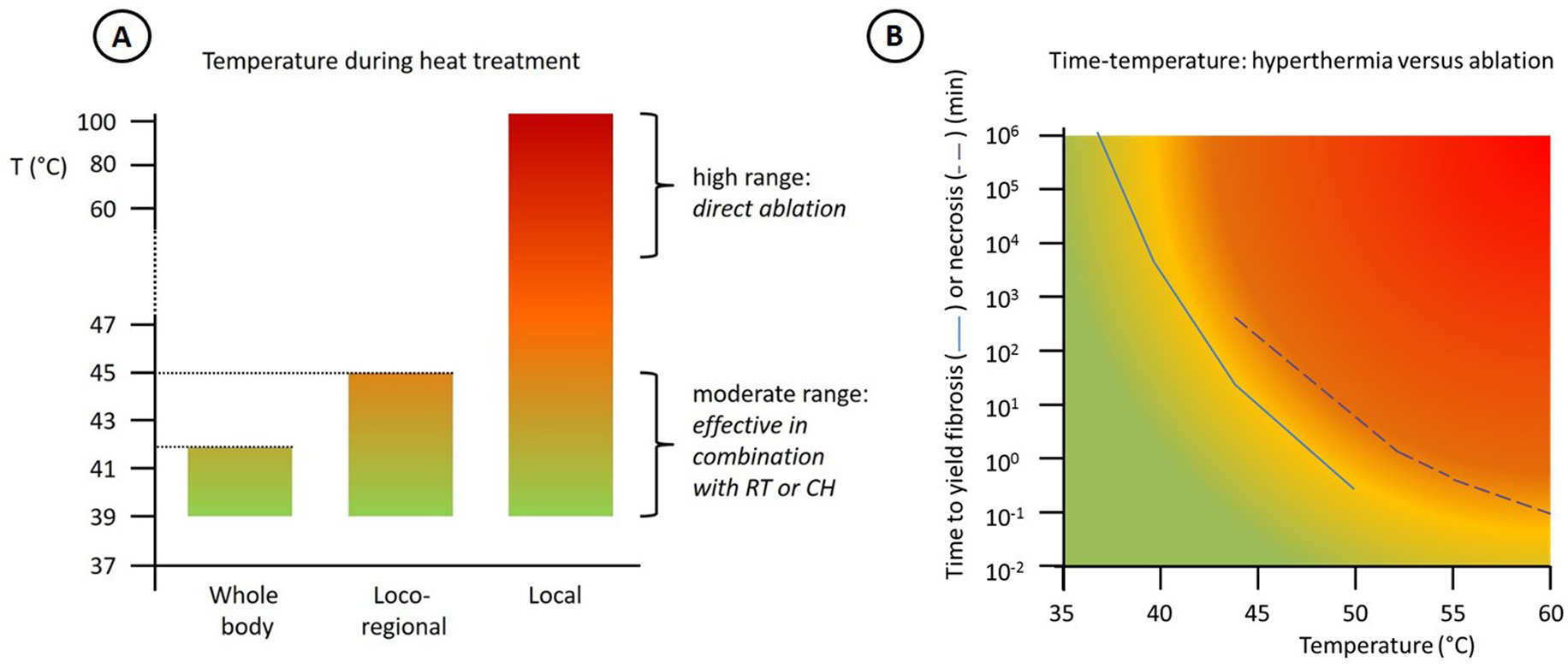
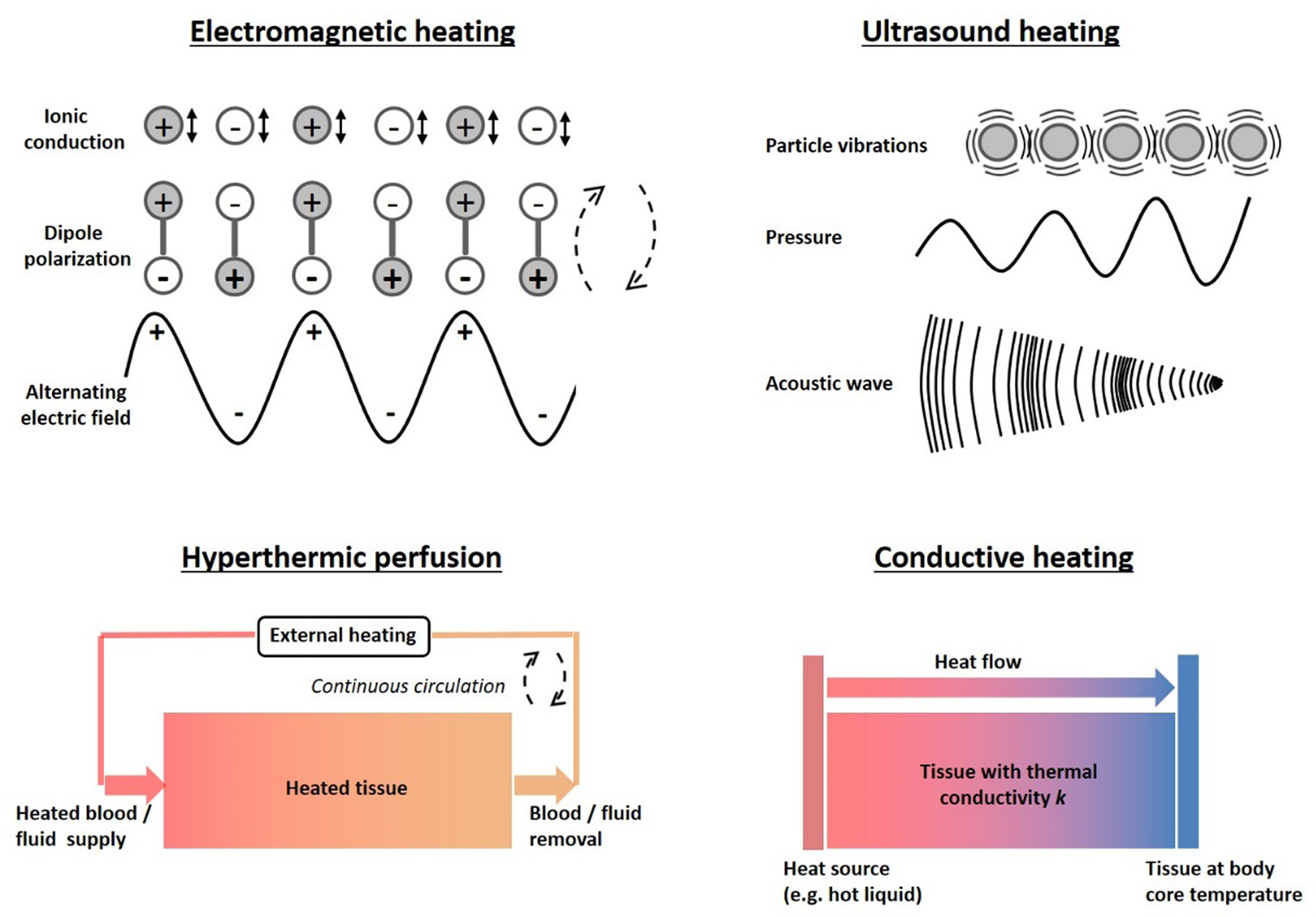
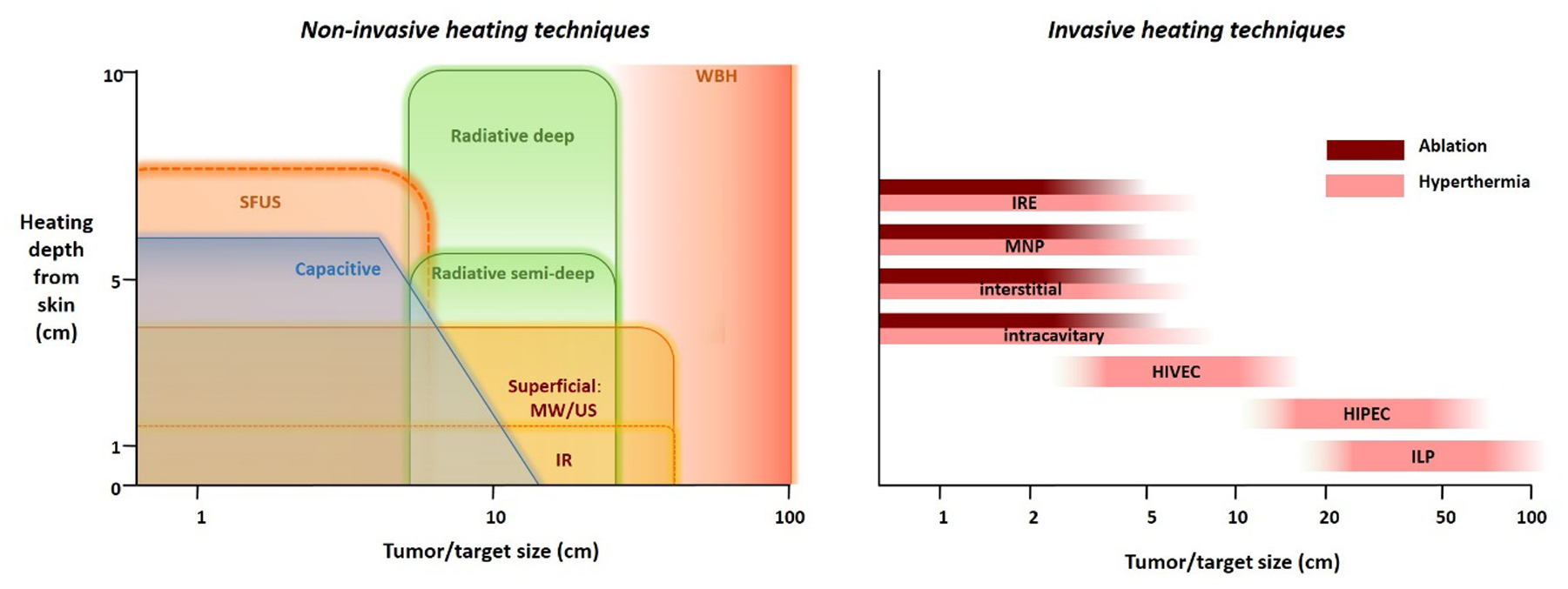
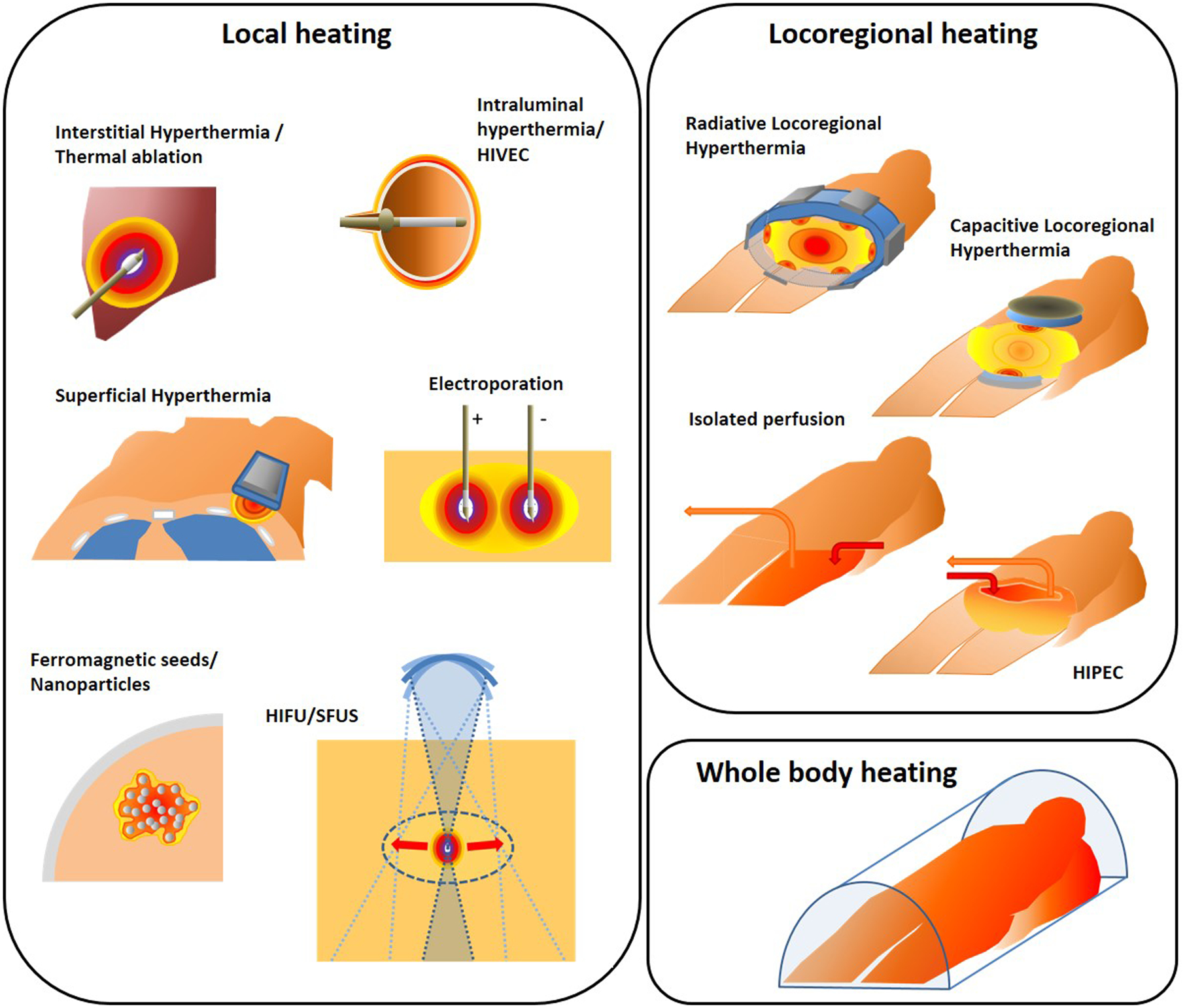
The therapeutic application of heat is very effective in cancer treatment. Both hyperthermia, i.e., heating to 39-45 °C to induce sensitization to radiotherapy and chemotherapy, and thermal ablation, where temperatures beyond 50 °C destroy tumor cells directly are frequently applied in the clinic. Achievement of an effective treatment requires high quality heating equipment, precise thermal dosimetry, and adequate quality assurance. Several types of devices, antennas and heating or power delivery systems have been proposed and developed in recent decades. These vary considerably in technique, heating depth, ability to focus, and in the size of the heating focus. Clinically used heating techniques involve electromagnetic and ultrasonic heating, hyperthermic perfusion and conductive heating. Depending on clinical objectives and available technology, thermal therapies can be subdivided into three broad categories: local, locoregional, or whole body heating. Clinically used local heating techniques include interstitial hyperthermia and ablation, high intensity focused ultrasound (HIFU), scanned focused ultrasound (SFUS), electroporation, nanoparticle heating, intraluminal heating and superficial heating. Locoregional heating techniques include phased array systems, capacitive systems and isolated perfusion. Whole body techniques focus on prevention of heat loss supplemented with energy deposition in the body, e.g., by infrared radiation. This review presents an overview of clinical hyperthermia and ablation devices used for local, locoregional, and whole body therapy. Proven and experimental clinical applications of thermal ablation and hyperthermia are listed. Methods for temperature measurement and the role of treatment planning to control treatments are discussed briefly, as well as future perspectives for heating technology for the treatment of tumors.
Keywords: HIPEC; ablation; heating equipment; hyhperthermia; thermal therapy.
Conflict of interest statement
Disclosure statement
R. Ivkov is an inventor on nanoparticle patents. All patents are assigned to either The Johns Hopkins University or Aduro BioTech, Inc. R. Ivkov consults for, and is a member of the Scientific Advisory Board for Imagion Biosystems, a company developing imaging with magnetic iron oxide nanoparticles. R. Ivkov also consults for Magnetic Insight, a company developing magnetic particle imaging. All other authors report no conflicts of interest. The contents of this paper are solely the responsibility of the authors.
Figures
References
-
- Coley WB, The treatment of malignant tumors by repeated inoculations of erysipelas. With a report of ten original cases. Am J Med Sci. 1893;105:487–511. - PubMed
-
- Rau B, Wust P, Tilly W, Gellermann J, Harder C, Riess H, Budach V, Felix R, and Schlag PM, Preoperative radiochemotherapy in locally advanced or recurrent rectal cancer: regional radiofrequency hyperthermia correlates with clinical parameters. Int J Radiat Oncol Biol Phys. 2000;48:381–91. - PubMed
-
- Kroesen M, Mulder HT, Van Holthe JML, Aangeenbrug AA, Mens JWM, Van Doorn HC, Paulides MM, Oomen-de Hoop E, Vernhout RM, Lutgens LC, Van Rhoon GC, and Franckena M, Confirmation of thermal dose as a predictor of local control in cervical carcinoma patients treated with state-of-the-art radiation therapy and hyperthermia. Radiother Oncol. 2019;140:150–158. - PubMed
-
- Bakker A, Van der Zee J, van tienhoven G, Kok HP, Rasch CRN, and Crezee H, Temperature and thermal dose during radiotherapy and hyperthermia for recurrent breast cancer are related to clinical outcome and thermal toxicity: A systematic review. Int J Hyperthermia. 2019;36:1024–1039. - PubMed
-
- van Rhoon GC, Is CEM43 still a relevant thermal dose parameter for hyperthermia treatment monitoring? Int J Hyperthermia. 2016;32:50–62. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical