

Femoral anteversion: significance and measurement
- PMID: 32579722
- PMCID: PMC7542196
- DOI: 10.1111/joa.13249
Femoral anteversion: significance and measurement
Abstract
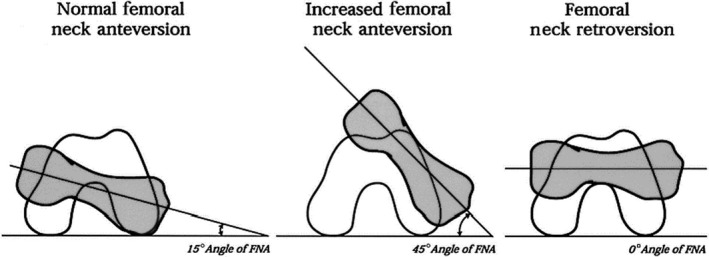
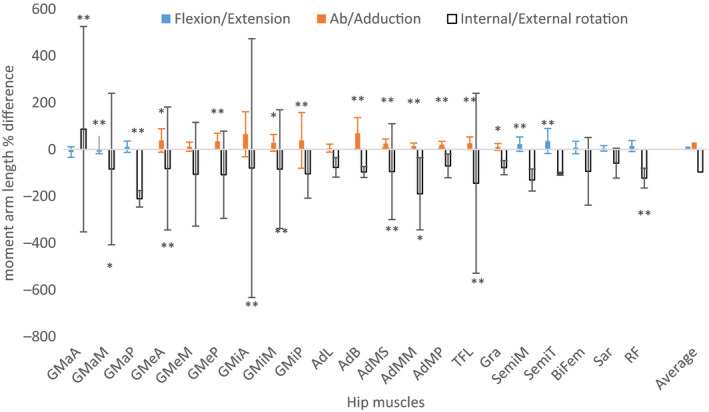
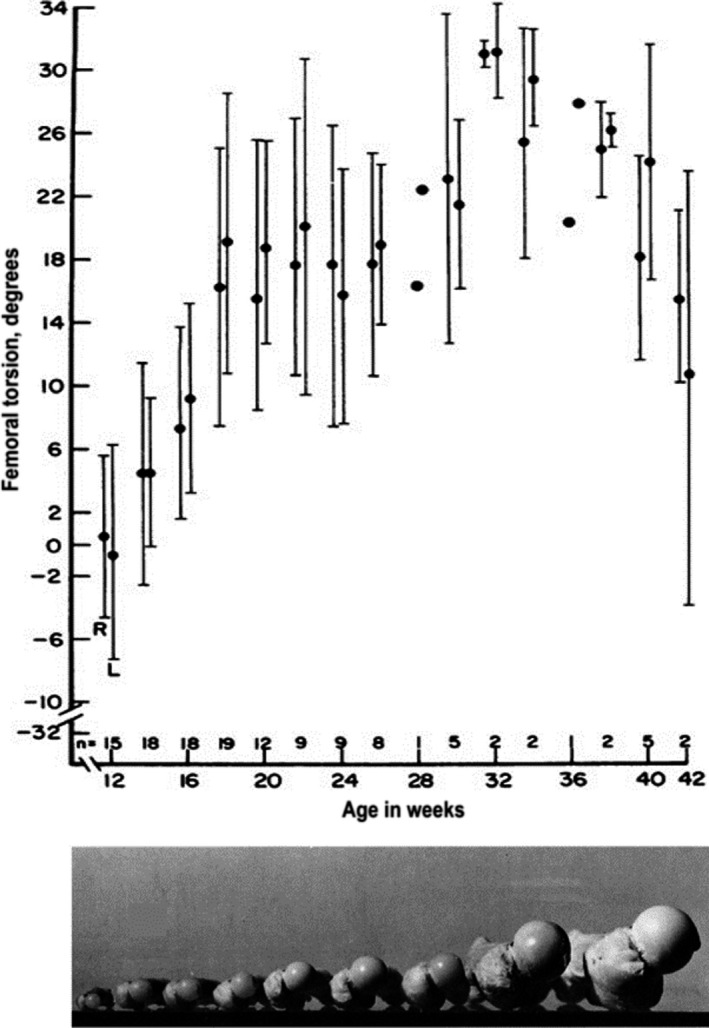
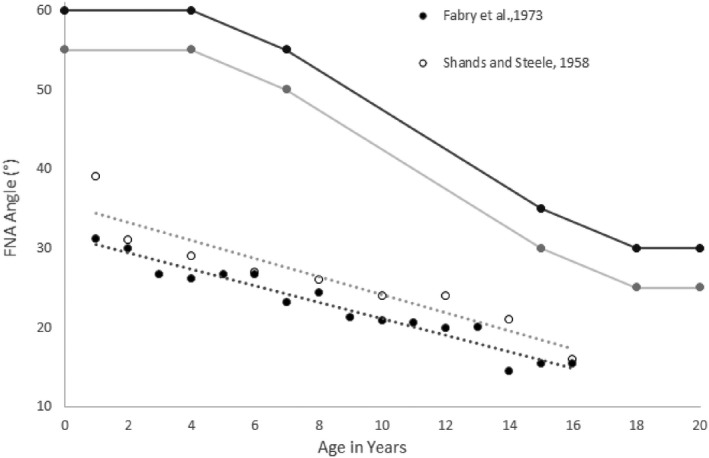
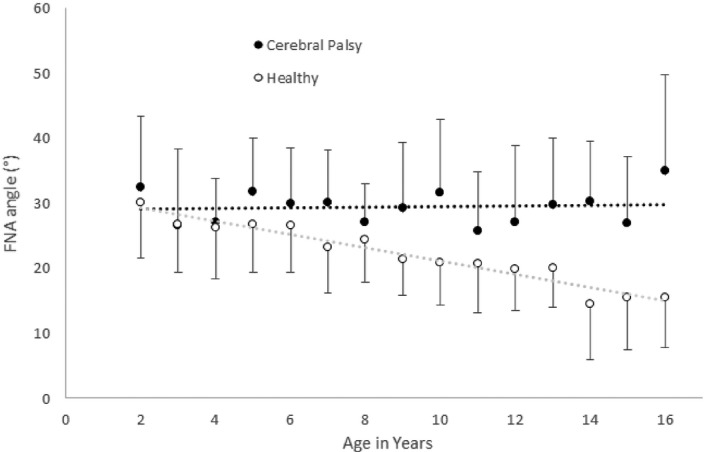
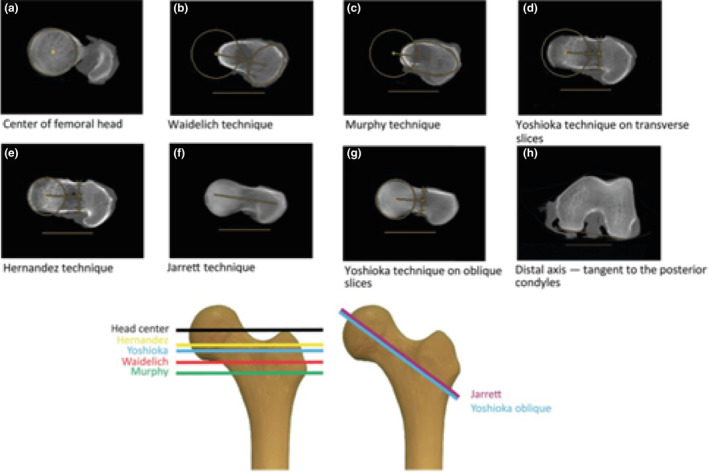
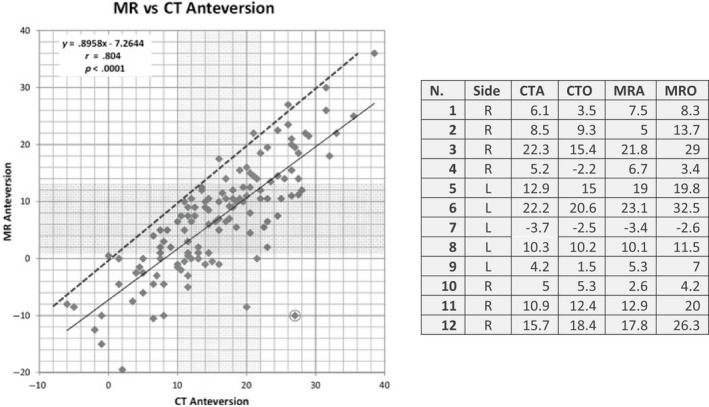
Femoral neck anteversion (FNA) is the angle between the femoral neck and femoral shaft, indicating the degree of torsion of the femur. Differences in FNA affect the biomechanics of the hip, through alterations in factors such as moment arm lengths and joint loading. Altered gait associated with differences in FNA may also contribute to the development of a wide range of skeletal disorders including osteoarthritis. FNA varies by up to 30° within apparently healthy adults. FNA increases substantially during gestation and thereafter decreases steadily until maturity. There is some evidence of a further decrease at a much lower rate during adulthood into old age, but the mechanisms behind it have never been studied. Development of FNA appears to be strongly influenced by mechanical forces experienced during everyday movements. This is evidenced by large differences in FNA in groups where movement is impaired, such as children born breech or individuals with neuromuscular conditions such as cerebral palsy. Several methods can be used to assess FNA, which may yield different values by up to 20° in the same participant. While MRI and CT are used clinically, limitations such as their cost, scanning time and exposure to ionising radiation limit their applicability in longitudinal and population studies, particularly in children. More broadly, applicable measures such as ultrasound and functional tests exist, but they are limited by poor reliability and validity. These issues highlight the need for a valid and reliable universally accepted method. Treatment for clinically problematic FNA is usually de-rotational osteotomy; passive, non-operative methods do not have any effect. Despite observational evidence for the effects of physical activity on FNA development, the efficacy of targeted physical activity remains unexplored. The aim of this review is to describe the biomechanical and clinical consequences of FNA, factors influencing FNA and the strengths and weaknesses of different methods used to assess FNA.
Keywords: antetorsion; hip; joint shape; proximal femur; skeletal development.
© 2020 The Authors. Journal of Anatomy published by John Wiley & Sons Ltd on behalf of Anatomical Society.
Conflict of interest statement
Matteo Scorcelletti, Neil Reeves, Jörn Rittweger and Alex Ireland declare that they have no conflict of interest.
Figures


References
-
- Aamodt, A. , Terjesen, T. , Eine, J. and Kvistad, K. (1995) Femoral anteversion measured by ultrasound and CT: a comparative study. Skeletal Radiology, 24, 105–109. - PubMed
-
- Aird, J. , Hogg, A. and Rollinson, P. (2009) Femoral torsion in patients with Blount's disease: a previously unrecognised component. The Journal of Bone and Joint Surgery, British, 91, 1388–1393. - PubMed
-
- Alvik, I. (1962) Increased anteversion of the femur as the only manifestation of dysplasia of the hip. Clinical Orthopaedics, 22, 16–20. - PubMed
-
- Amraee, D. , Alizadeh, M. , Minoonejhad, H. , Razi, M. and Amraee, G. (2017) Predictor factors for lower extremity malalignment and non‐contact anterior cruciate ligament injuries in male athletes. Knee Surgery, Sports Traumatology, Arthroscopy, 25, 1625–1631. - PubMed
-
- Anda, S. , Terjesen, T. , Kvistad, K.A. and Svenningsen, S. (1991) Acetabular angles and femoral anteversion in dysplastic hips in adults: CT investigation. Journal of Computer Assisted Tomography, 15, 115–120. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
