

Effect on Patient Safety of a Resident Physician Schedule without 24-Hour Shifts
- PMID: 32579812
- PMCID: PMC7405505
- DOI: 10.1056/NEJMoa1900669
Effect on Patient Safety of a Resident Physician Schedule without 24-Hour Shifts
Abstract
Background: The effects on patient safety of eliminating extended-duration work shifts for resident physicians remain controversial.
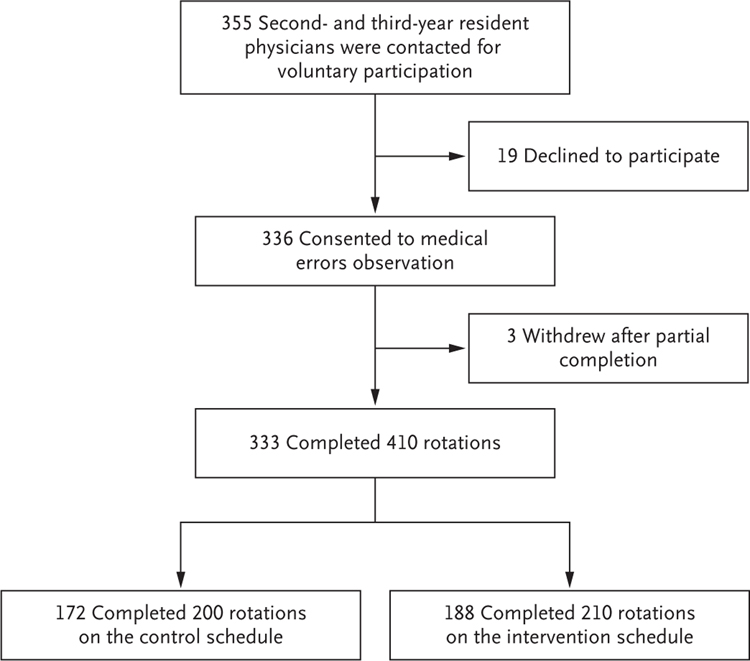
Methods: We conducted a multicenter, cluster-randomized, crossover trial comparing two schedules for pediatric resident physicians during their intensive care unit (ICU) rotations: extended-duration work schedules that included shifts of 24 hours or more (control schedules) and schedules that eliminated extended shifts and cycled resident physicians through day and night shifts of 16 hours or less (intervention schedules). The primary outcome was serious medical errors made by resident physicians, assessed by intensive surveillance, including direct observation and chart review.
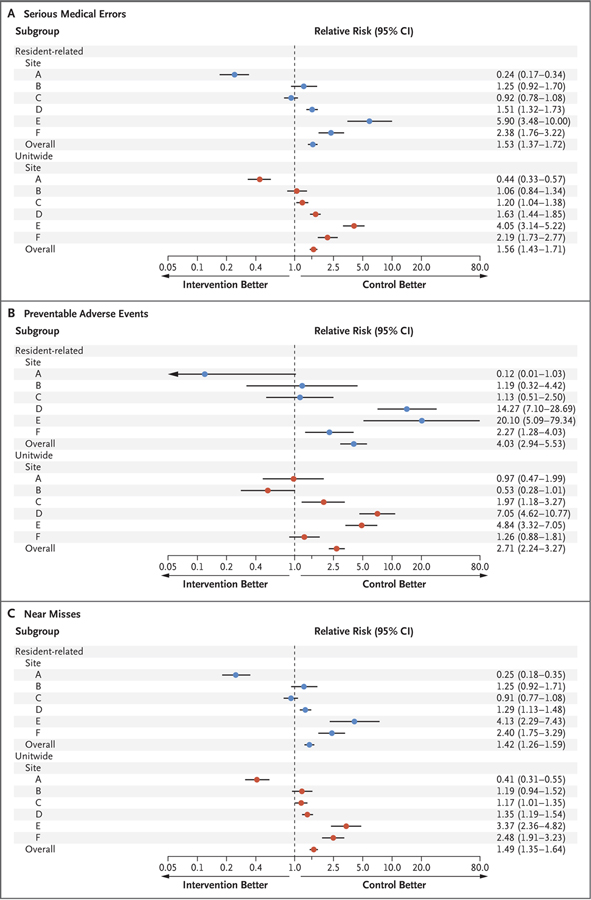
Results: The characteristics of ICU patients during the two work schedules were similar, but resident physician workload, described as the mean (±SD) number of ICU patients per resident physician, was higher during the intervention schedules than during the control schedules (8.8±2.8 vs. 6.7±2.2). Resident physicians made more serious errors during the intervention schedules than during the control schedules (97.1 vs. 79.0 per 1000 patient-days; relative risk, 1.53; 95% confidence interval [CI], 1.37 to 1.72; P<0.001). The number of serious errors unitwide were likewise higher during the intervention schedules (181.3 vs. 131.5 per 1000 patient-days; relative risk, 1.56; 95% CI, 1.43 to 1.71). There was wide variability among sites, however; errors were lower during intervention schedules than during control schedules at one site, rates were similar during the two schedules at two sites, and rates were higher during intervention schedules than during control schedules at three sites. In a secondary analysis that was adjusted for the number of patients per resident physician as a potential confounder, intervention schedules were no longer associated with an increase in errors.
Conclusions: Contrary to our hypothesis, resident physicians who were randomly assigned to schedules that eliminated extended shifts made more serious errors than resident physicians assigned to schedules with extended shifts, although the effect varied by site. The number of ICU patients cared for by each resident physician was higher during schedules that eliminated extended shifts. (Funded by the National Heart, Lung, and Blood Institute; ROSTERS ClinicalTrials.gov number, NCT02134847.).
Copyright © 2020 Massachusetts Medical Society.
Figures
Comment in
-
Re: Effect on Patient Safety of a Resident Physician Schedule without 24-Hour Shifts.J Urol. 2020 Nov;204(5):1086-1087. doi: 10.1097/JU.0000000000001256.01. Epub 2020 Sep 8. J Urol. 2020. PMID: 32897125 No abstract available.
-
Patient Safety and Resident Schedules without 24-Hour Shifts.N Engl J Med. 2020 Sep 24;383(13):1286. doi: 10.1056/NEJMc2025843. N Engl J Med. 2020. PMID: 32966728 No abstract available.
-
Patient Safety and Resident Schedules without 24-Hour Shifts.N Engl J Med. 2020 Sep 24;383(13):1286-1287. doi: 10.1056/NEJMc2025843. N Engl J Med. 2020. PMID: 32966729 No abstract available.
-
Patient Safety and Resident Schedules without 24-Hour Shifts.N Engl J Med. 2020 Sep 24;383(13):1287. doi: 10.1056/NEJMc2025843. N Engl J Med. 2020. PMID: 32966730 No abstract available.
-
Patient Safety and Resident Schedules without 24-Hour Shifts.N Engl J Med. 2020 Sep 24;383(13):1287. doi: 10.1056/NEJMc2025843. N Engl J Med. 2020. PMID: 32966731 No abstract available.
-
Physician schedules and patient safety: Critical appraisal.Natl Med J India. 2020 Nov-Dec;33(6):359-361. doi: 10.4103/0970-258X.321146. Natl Med J India. 2020. PMID: 34341215 No abstract available.
References
-
- Friedman RC, Bigger JT, Kornfeld DS. The intern and sleep loss. N Engl J Med 1971;285:201–3. - PubMed
-
- Philibert I Sleep loss and performance in residents and nonphysicians: a meta-analytic examination. Sleep 2005;28:1392–402. - PubMed
-
- Eastridge BJ, Hamilton EC, O’Keefe GE, et al. Effect of sleep deprivation on the performance of simulated laparoscopic surgical skill. Am J Surg 2003;186:169–74. - PubMed
-
- Gaba DM, Howard SK. Patient safety: fatigue among clinicians and the safety of patients. N Engl J Med 2002;347:1249–55. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
- HFP-04201/National Space Biomedical Research Institute/International
- HFP-0006/National Space Biomedical Research Institute/International
- K24 HL105664/HL/NHLBI NIH HHS/United States
- HFP-02802/National Space Biomedical Research Institute/International
- K24-HL-105664/HL/NHLBI NIH HHS/United States
- U01-HL-111691/HL/NHLBI NIH HHS/United States
- R01-HL-128538/HL/NHLBI NIH HHS/United States
- U01 HL111478/HL/NHLBI NIH HHS/United States
- R01-OH-010300/OH/NIOSH CDC HHS/United States
- R21-HD-086392/National Institute of Child Health and Human Development/International
- R01-GM-105018/GM/NIGMS NIH HHS/United States
- R01-HL-114088/HL/NHLBI NIH HHS/United States
- U01-HL-111478/HL/NHLBI NIH HHS/United States
- R01 OH010300/OH/NIOSH CDC HHS/United States
- R01 OH011773/OH/NIOSH CDC HHS/United States
- P01-AG-009975/AG/NIA NIH HHS/United States
- U01 HL111691/HL/NHLBI NIH HHS/United States