

Diagnostic accuracy of the FebriDx host response point-of-care test in patients hospitalised with suspected COVID-19
- PMID: 32579983
- PMCID: PMC7306108
- DOI: 10.1016/j.jinf.2020.06.051
Diagnostic accuracy of the FebriDx host response point-of-care test in patients hospitalised with suspected COVID-19
Abstract
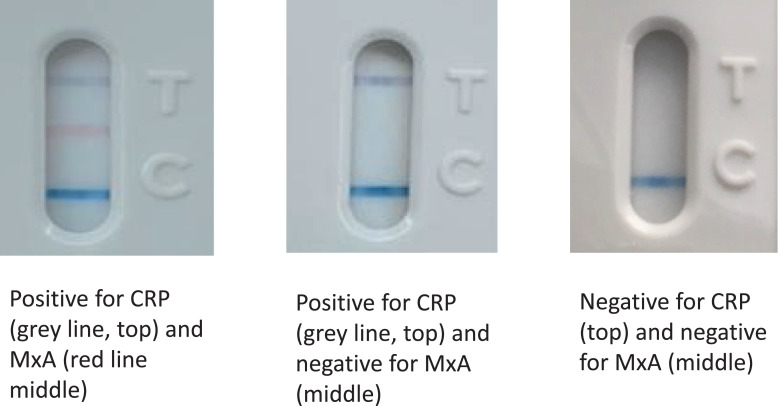
Introduction: Management of the COVID-19 pandemic is hampered by long delays associated with centralised laboratory PCR testing. In hospitals this leads to poor patient flow and nosocomial transmission and so rapid, accurate diagnostic tests are urgently required. The FebriDx is a point-of-care test that detects an antiviral host response protein in finger prick blood within 10 min, but its accuracy for the identification of COVID-19 is unknown.
Methods: We performed a real-world diagnostic accuracy study of FebriDx in hospitalised patients during the first wave of the pandemic. Measures of diagnostic accuracy were calculated based on FebriDx results compared to the reference standard of SARS-CoV-2 PCR on combined nose and throat swabs. A multivariable predictive model including FebriDx, age, sex, and clinical characteristics was developed and underwent internal validation.
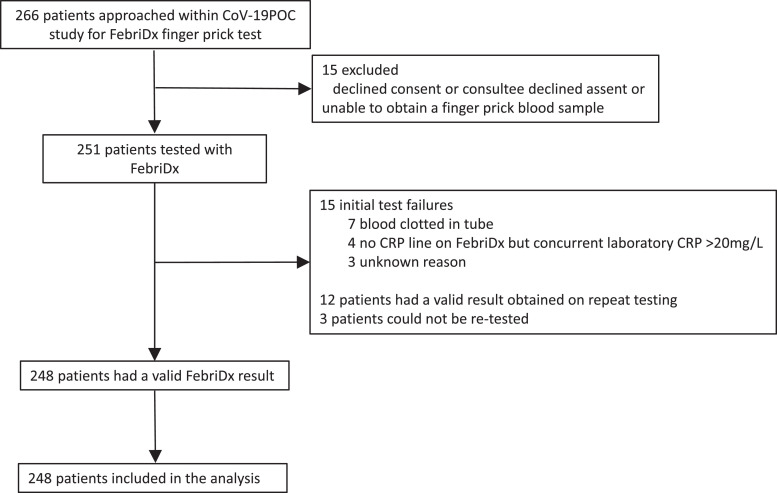
Results: FebriDx was performed on 251 patients and gave a valid result in 248. 118 of 248 (48%) were PCR positive for COVID-19. FebriDx results were available after 10 min compared with 1.7 (1.6 to 2.1) hours with point-of-care PCR testing and 23.4 (17.2 to 31.1) hours with laboratory PCR testing. Sensitivity of FebriDx for the identification of COVID-19 was 93% (110/118; 95% CI 87 to 97%) and specificity was 86% (112/130; 95%CI 79 to 92%). Positive and negative likelihood ratios were 6.73 (95%CI 4.37 to 10.37) and 0.08 (95%CI 0.04 to 0.15) respectively. In the multivariate model age, sex and other clinical features did not contribute significantly to the effect of the FebriDx result in distinguishing patients with and without COVID-19.
Conclusions: During the first wave of the pandemic, FebriDx had high accuracy for the identification of COVID-19 in hospitalised adults and could be deployed as a front door triage tool.
Trial registration: ISRCTN14966673.
Keywords: Accuracy; COVID-19; Host response; MxA; Point of care testing; SARS-CoV-2.
Copyright © 2020 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Declaration of Competing Interest TWC has received speaker fees, honoraria, travel reimbursement, and equipment and consumables free of charge for the purposes of research outside of this submitted study, from BioFire diagnostics LLC and BioMerieux. TWC has received consultancy fees from Synairgen research Ltd, Randox laboratories Ltd and Cidara therapeutics. He a member of an advisory board for Roche and a member of two independent data monitoring committees for trials sponsored by Roche. He has acted as the UK chief investigator for an IMP study sponsored by Janssen. All other authors have completed the Unified Competing Interest form (available on request from the corresponding author) and declare: no support from any organisation for the submitted work no financial relationships with any organisations that might have an interest in the submitted work in the previous three years, no other relationships or activities that could appear to have influenced the submitted work.
Figures
Comment in
-
A model to identify individuals with a high probability of a SARS-CoV-2 infection.J Infect. 2021 Mar;82(3):e32-e34. doi: 10.1016/j.jinf.2020.11.028. Epub 2020 Nov 25. J Infect. 2021. PMID: 33245942 Free PMC article. No abstract available.
-
Myxovirus resistance protein A in peripheral blood predicts supplemental oxygen need in COVID-19.J Infect. 2021 May;82(5):186-230. doi: 10.1016/j.jinf.2020.12.006. Epub 2020 Dec 8. J Infect. 2021. PMID: 33307140 Free PMC article. No abstract available.
References
-
- Nakabayashi M., Adachi Y., Itazawa T., Okabe Y., Kanegane H., Kawamura M., Tomita A., Miyawaki T. MxA-based recognition of viral illness in febrile children by a whole blood assay. Pediatr Res. 2006;60:770–774. - PubMed
-
- Engelmann I., Dubos F., Lobert P.E., Houssin C., Degas V., Sardet A., Decoster A., Dewilde A., Martinot A., Hober D. Diagnosis of viral infections using myxovirus resistance A (MxA) Pediatrics. 2015;135:e985–e993. - PubMed
-
- Shapiro N.I., Self W.H., Rosen J., Sharo S.C., Filbin M.R., Hou P.C., Parekh A.D., Kurz M., Sambursky R. A prospective, multi-centre US clinical trial to determine accuracy of FebriDx point-of-care testing for acute upper respiratory infections with and without a confirmed fever. Ann Med. 2018;18:1–10. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
