Patterns of practice for adaptive and real-time radiation therapy (POP-ART RT) part II: Offline and online plan adaption for interfractional changes
- PMID: 32579998
- PMCID: PMC7758781
- DOI: 10.1016/j.radonc.2020.06.017
Patterns of practice for adaptive and real-time radiation therapy (POP-ART RT) part II: Offline and online plan adaption for interfractional changes
Abstract
Purpose: The POP-ART RT study aims to determine to what extent and how intrafractional real-time respiratory motion management (RRMM), and plan adaptation for interfractional anatomical changes (ART) are used in clinical practice and to understand barriers to implementation. Here we report on part II: ART using more than one plan per target per treatment course.
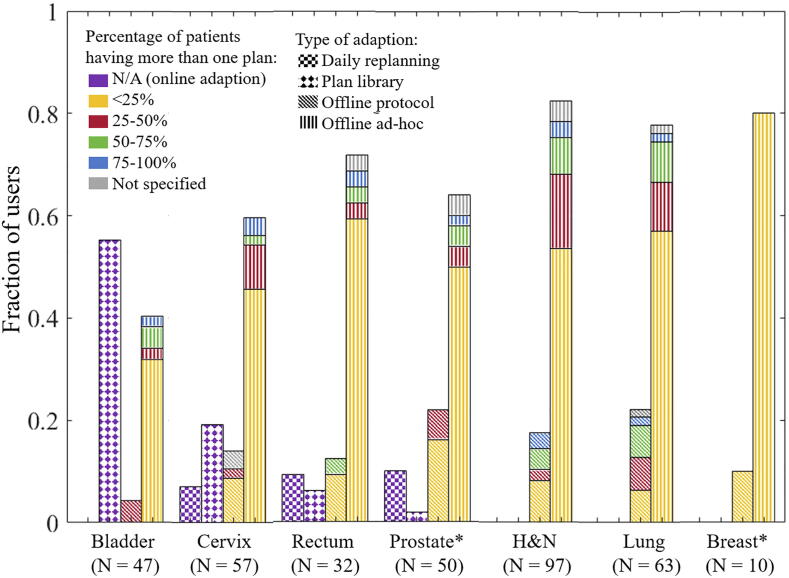
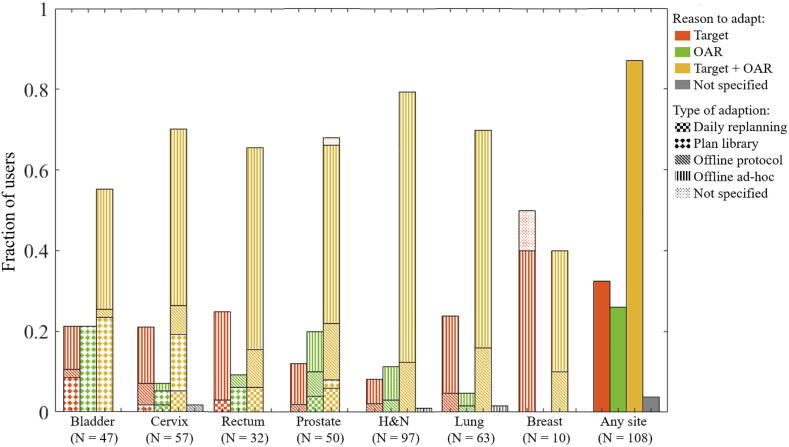
Materials and methods: A questionnaire on the current practice of ART, wishes for expansion or implementation, and barriers to implementation was distributed worldwide. Four types of ART were discriminated: daily online replanning, online plan library, protocolled offline replanning (all three based on a protocol), and ad-hoc offline replanning.
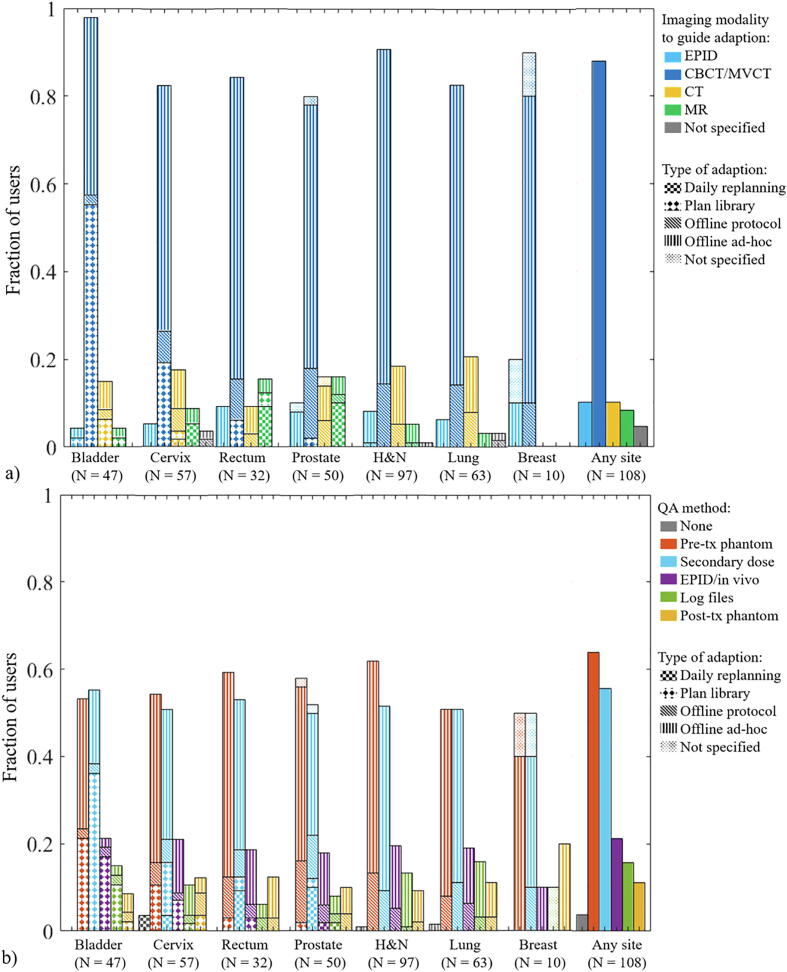
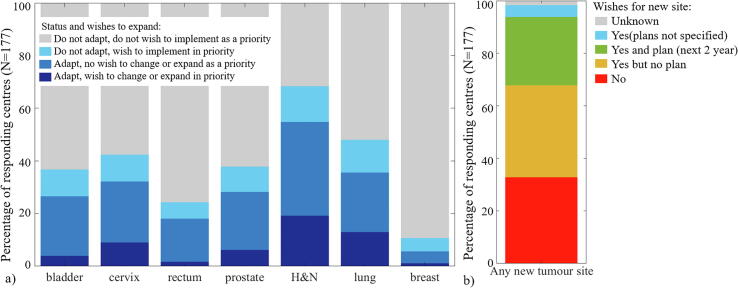
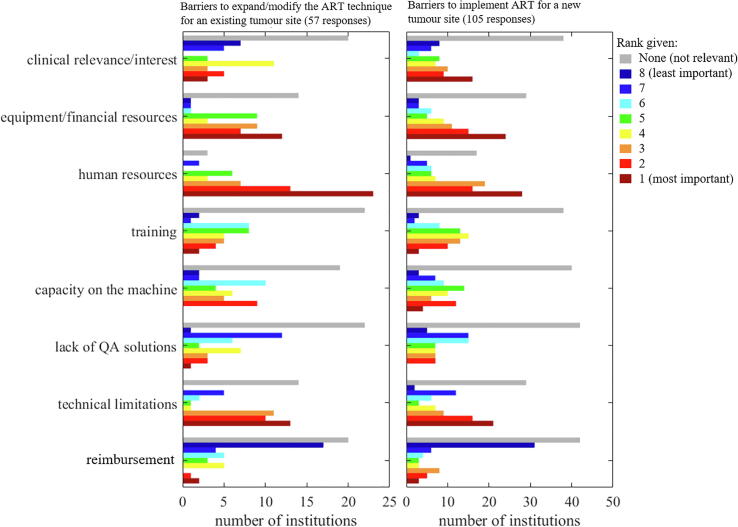
Results: The questionnaire was completed by 177 centres from 40 countries. ART was used by 61% of respondents (31% with protocol) for a median (range) of 3 (1-8) tumour sites. CBCT/MVCT was the main imaging modality except for online daily replanning (11 users) where 10 users used MR. Two thirds of respondents wished to implement ART for a new tumour site; 40% of these had plans to do it in the next 2 years. Human/material resources and technical limitations were the main barriers to further use and implementation.
Conclusions: ART was used for a broad range of tumour sites, mainly with ad-hoc offline replanning and for a median of 3 tumour sites. There was a large interest in implementing ART for more tumour sites, mainly limited by human/material resources and technical limitations. Daily online replanning was primarily performed on MR-linacs.
Keywords: Adaptive radiotherapy; Image-guided radiotherapy (IGRT); Interfractional motion; MR-guided radiotherapy; Plan library; Plan of the day.
Copyright © 2020 The Authors. Published by Elsevier B.V. All rights reserved.
Figures