

Nanoscale regulation of L-type calcium channels differentiates between ischemic and dilated cardiomyopathies
- PMID: 32580140
- PMCID: PMC7317229
- DOI: 10.1016/j.ebiom.2020.102845
Nanoscale regulation of L-type calcium channels differentiates between ischemic and dilated cardiomyopathies
Abstract
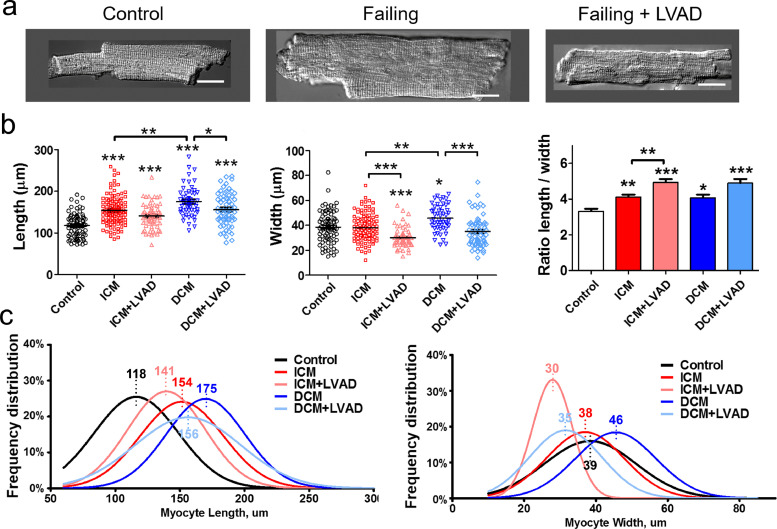
Background: Subcellular localization and function of L-type calcium channels (LTCCs) play an important role in regulating contraction of cardiomyocytes. Understanding how this is affected by the disruption of transverse tubules during heart failure could lead to new insights into the disease.
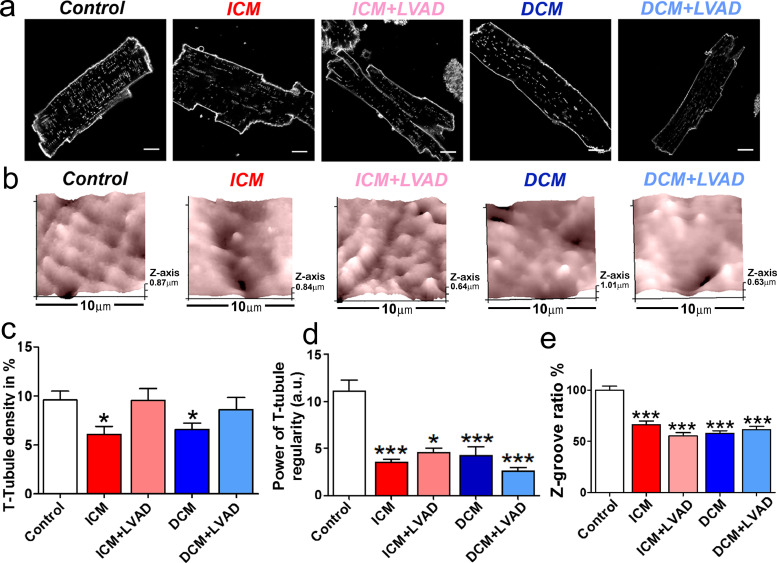
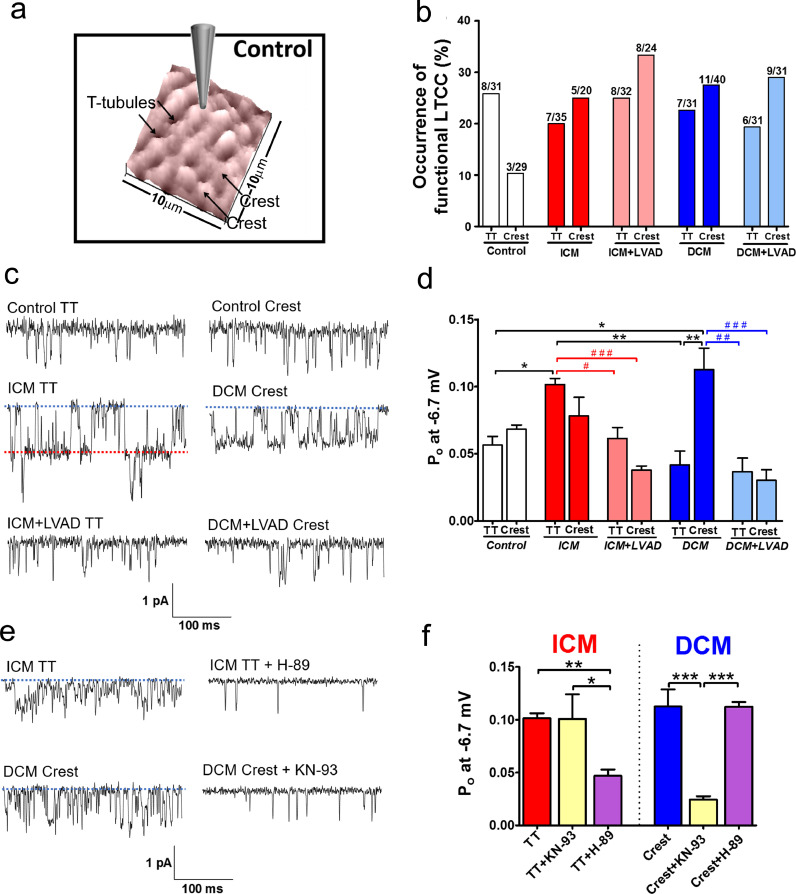
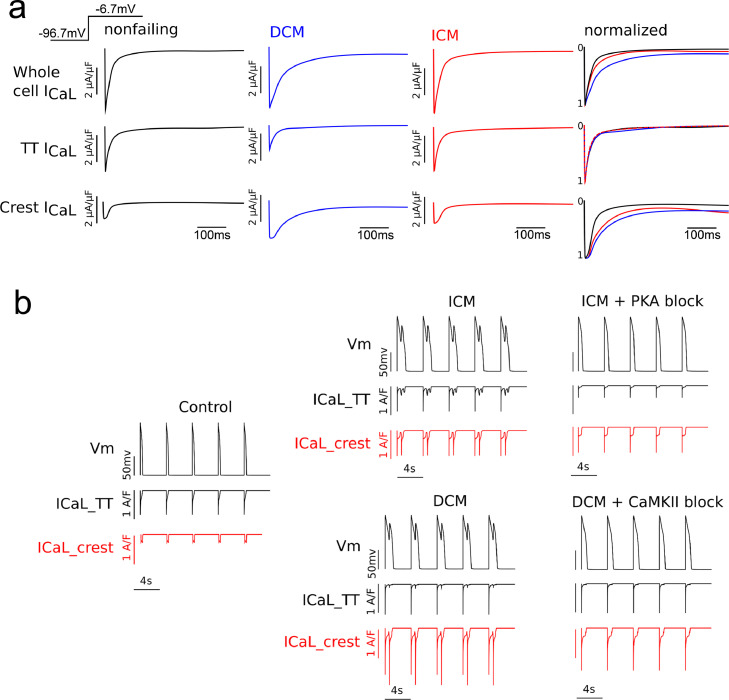
Methods: Cardiomyocytes were isolated from healthy donor hearts, as well as from patients with cardiomyopathies and with left ventricular assist devices. Scanning ion conductance and confocal microscopy was used to study membrane structures in the cells. Super-resolution scanning patch-clamp was used to examine LTCC function in different microdomains. Computational modeling predicted the impact of these changes to arrhythmogenesis at the whole-heart level.
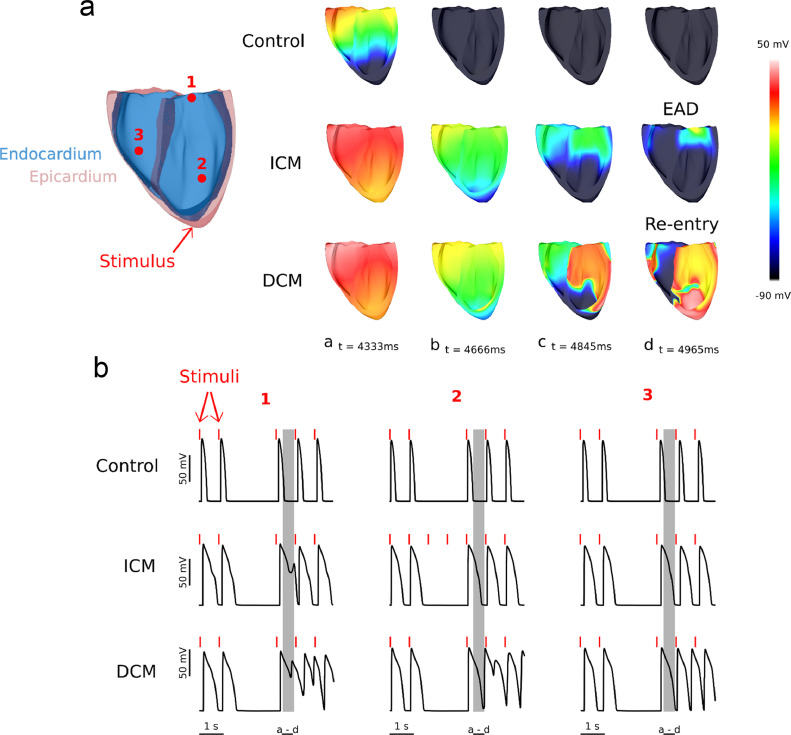
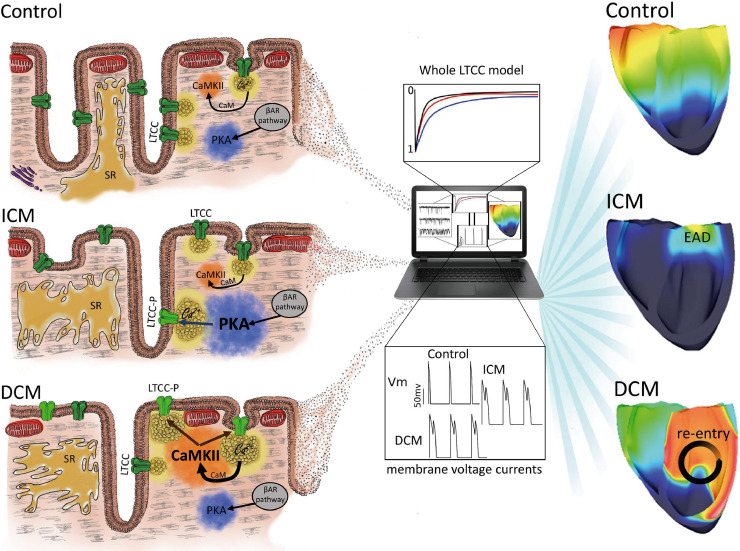
Findings: We showed that loss of structural organization in failing myocytes leads to re-distribution of functional LTCCs from the T-tubules to the sarcolemma. In ischemic cardiomyopathy, the increased LTCC open probability in the T-tubules depends on the phosphorylation by protein kinase A, whereas in dilated cardiomyopathy, the increased LTCC opening probability in the sarcolemma results from enhanced phosphorylation by calcium-calmodulin kinase II. LVAD implantation corrected LTCCs pathophysiological activity, although it did not improve their distribution. Using computational modeling in a 3D anatomically-realistic human ventricular model, we showed how LTCC location and activity can trigger heart rhythm disorders of different severity.
Interpretation: Our findings demonstrate that LTCC redistribution and function differentiate between disease aetiologies. The subcellular changes observed in specific microdomains could be the consequence of the action of distinct protein kinases.
Funding: This work was supported by NIH grant (ROI-HL 126802 to NT-JG) and British Heart Foundation (grant RG/17/13/33173 to JG, project grant PG/16/17/32069 to RAC). Funders had no role in study design, data collection, data analysis, interpretation, writing of the report.
Keywords: Cardiomyopathy; Computational biology; Electrophysiology; Heart Failure; Ion channels.
Copyright © 2020 The Authors. Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
Declaration of Competing Interest The authors declare no competing interests.
Figures
References
-
- Tomaselli G.F. What causes sudden death in heart failure? Circ Res. 2004;95:754–763. - PubMed
-
- Al Chekakie M.O. Traditional heart failure medications and sudden cardiac death prevention: a review. J Cardiovasc Pharmacol Ther. 2013;18:412–426. - PubMed
-
- Bers D.M. Calcium cycling and signaling in cardiac myocytes. Annu Rev Physiol. 2008;70:23–49. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
