

Pulmonary Hypertension Phenotypes in Systemic Sclerosis: The Right Diagnosis for the Right Treatment
- PMID: 32580360
- PMCID: PMC7352262
- DOI: 10.3390/ijms21124430
Pulmonary Hypertension Phenotypes in Systemic Sclerosis: The Right Diagnosis for the Right Treatment
Abstract
Systemic sclerosis is an auto-immune disease characterized by skin involvement that often affects multiple organ systems. Pulmonary hypertension is a common finding that can significantly impact prognosis. Molecular pathophysiological mechanisms underlying pulmonary hypertension in systemic sclerosis can be extremely heterogeneous, leading to distinct clinical phenotypes. In addition, different causes of pulmonary hypertension may overlap within the same patient. Since pulmonary hypertension treatment is very different for each phenotype, it is fundamental to perform an adequate diagnostic work-up to properly and promptly identify the prevalent mechanism underlying pulmonary hypertension in order to start the right therapies. When pulmonary hypertension is caused by a primary vasculopathy of the small pulmonary arteries, treatment with pulmonary vasodilators, often in an initial double-combination regimen, is indicated, aimed at reducing the mortality risk profile. In this review, we describe the different clinical phenotypes of pulmonary hypertension in the scleroderma population and discuss the utility of clinical tools to identify the presence of pulmonary vascular disease. Furthermore, we focus on systemic sclerosis-associated pulmonary arterial hypertension, highlighting the advances in the knowledge of right ventricular dysfunction in this setting and the latest updates in terms of treatment with pulmonary vasodilator drugs.
Keywords: pulmonary hypertension; pulmonary vascular disease; pulmonary vasodilators; risk stratification; systemic sclerosis.
Conflict of interest statement
The Authors declare no conflict of interest.
Figures

References
-
- Hachulla E., De Groote P., Gressin V., Sibilia J., Diot E., Carpentier P., Mouthon L., Hatron P.Y., Jego P., Allanore Y., et al. The three-year incidence of pulmonary arterial hypertension associated with systemic sclerosis in a multicenter nationwide longitudinal study in France. Arthritis Rheum. 2009;60:1831–1839. doi: 10.1002/art.24525. - DOI - PubMed
-
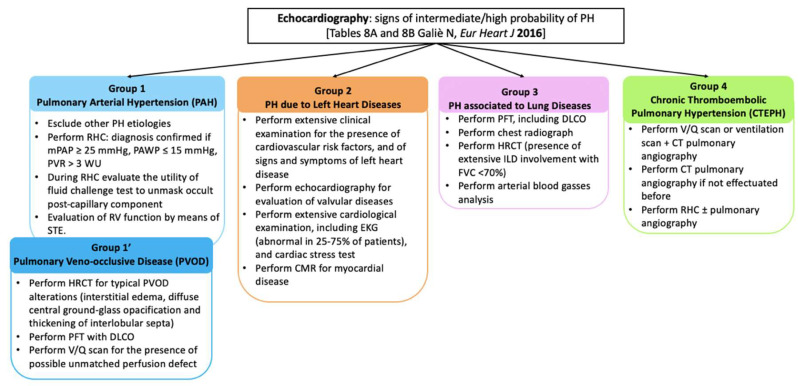
- Galiè N., Humbert M., Vachiery J.-L., Gibbs S., Lang I., Torbicki A., Simonneau G., Peacock A., Vonk Noordegraaf A., Beghetti M., et al. 2015 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension: The Joint Task Force for the Diagnosis and Treatment of Pulmonary Hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS): Endo. Eur. Heart J. 2016;37:67–119. doi: 10.1093/eurheartj/ehv317. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
