

Vogt-Koyanagi-Harada disease-like uveitis following nivolumab administration treated with steroid pulse therapy: a case report
- PMID: 32580711
- PMCID: PMC7313170
- DOI: 10.1186/s12886-020-01519-5
Vogt-Koyanagi-Harada disease-like uveitis following nivolumab administration treated with steroid pulse therapy: a case report
Abstract
Background: Immune checkpoint inhibitors can cause various adverse effects. Recently it has been shown that Vogt-Koyanagi-Harada (VKH) disease-like uveitis can occur in patients treated with nivolumab.
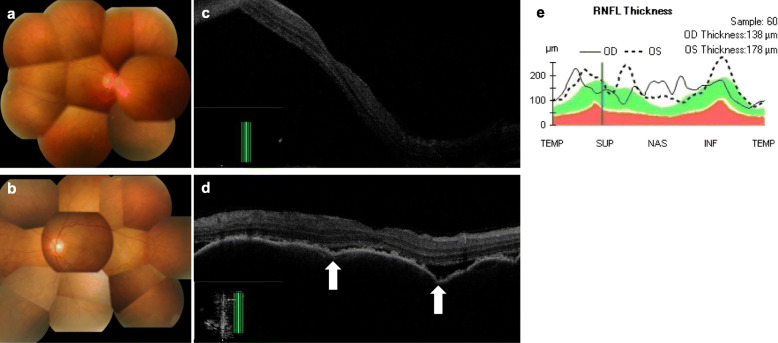
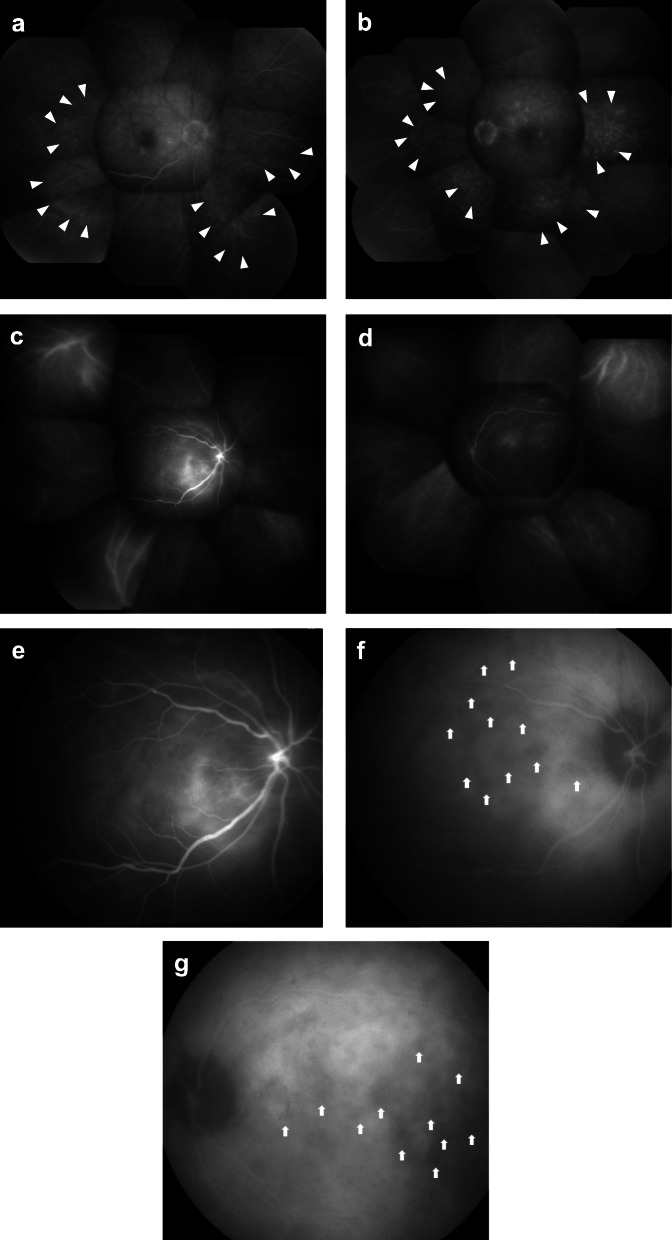
Case presentation: A 69-year-old man developed bilateral panuveitis after nivolumab treatment for recurrent hypopharyngeal cancer. Slit lamp examination revealed bilateral granulomatous keratic precipitates, anterior chamber cells and partial synechiae. Fundus examination revealed bilateral optic disc edema and diffuse serous retinal detachment. His human leukocyte antigen (HLA) typing showed HLA-DRB1*04:05 allele. A lumbar puncture did not demonstrate pleocytosis. Bilateral sub-tenon injections of triamcinolone acetonide were initiated. As his panuveitis did not regress completely, steroid pulse therapy was administered. That therapy led to the resolution of his serous retinal detachment and to rapid improvement in his vision. Following this, we treated him with 50 mg/day of prednisolone for 1 week and then reduced it by 5 mg every week. No bilateral uveitis relapse had occurred by his 3-month follow-up; however, he subsequently died because of his cancer.
Conclusion: To our knowledge, this is the first report of a patient with NVKH who underwent a lumbar puncture. Unlike VKH, our case did not show meningismus or pleocytosis. NVKH may, therefore, have a different etiology from VKH. In cases of NVKH with posterior uveitis, steroid pulse therapy may be considered as a treatment option, as it is in VKH.
Keywords: Examination of cerebrospinal fluid; HLA-DR4; Immune checkpoint inhibitors; Immune related adverse events; Nivolumab; PD-1 inhibitor; Steroid pulse therapy; Vogt–Koyanagi–Harada disease.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
