

The impact of gravidity, symptomatology and timing of infection on placental malaria
- PMID: 32580739
- PMCID: PMC7315526
- DOI: 10.1186/s12936-020-03297-3
The impact of gravidity, symptomatology and timing of infection on placental malaria
Abstract
Background: Placental malaria is associated with increased risk of adverse perinatal outcomes. While primigravidity has been reported as a risk factor for placental malaria, little is known regarding the relationship between gravidity, symptomatology and timing of Plasmodium falciparum infection and the development of placental malaria.
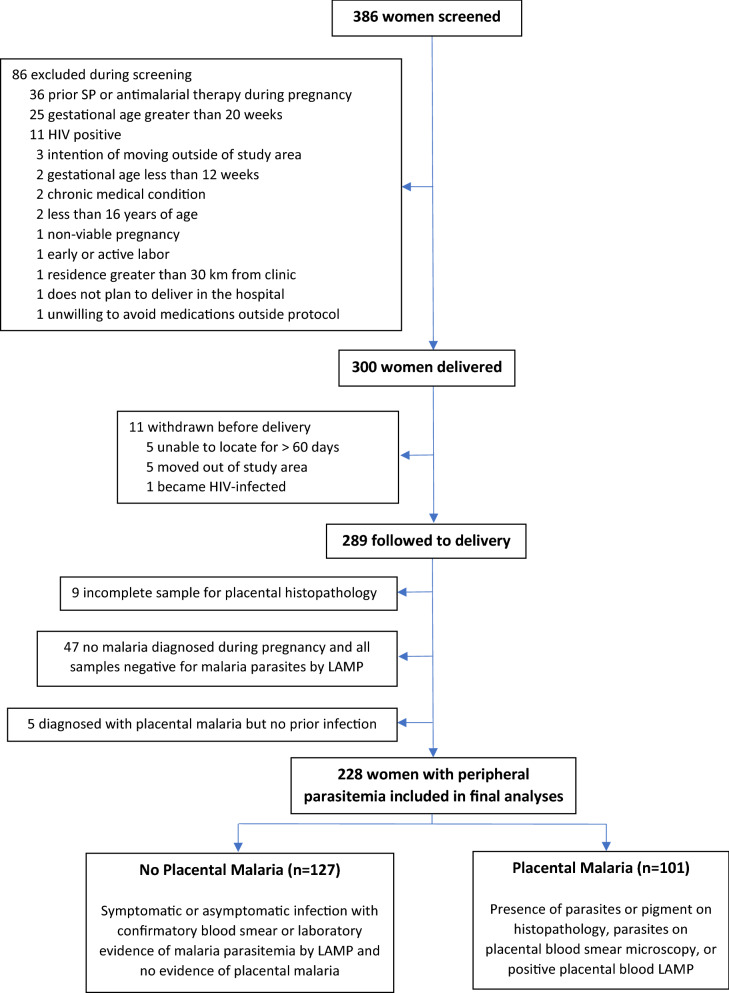
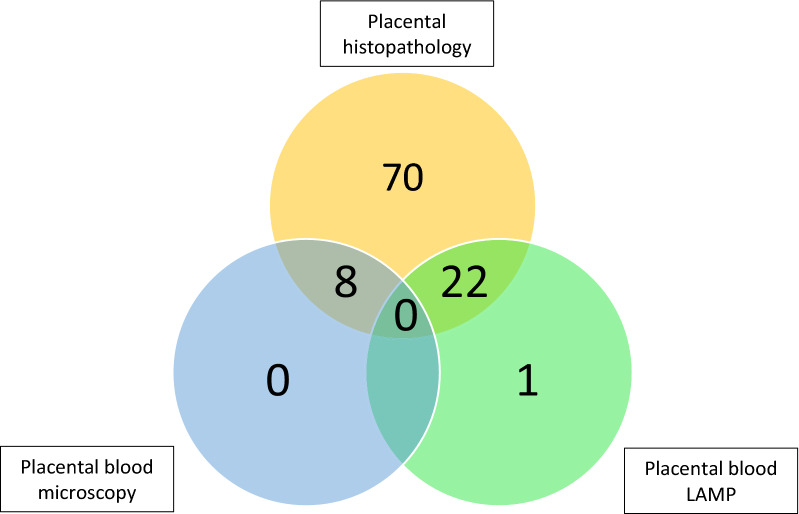
Methods: The aim of this study was to investigate the relationship between the development of placental malaria and gravidity, timing of infection, and presence of symptoms. This is a secondary analysis of data from a double-blind randomized control trial of intermittent preventive therapy during pregnancy in Uganda. Women were enrolled from 12 to 20 weeks gestation and followed through delivery. Exposure to malaria parasites was defined as symptomatic (fever with positive blood smear) or asymptomatic (based on molecular detection of parasitaemia done routinely every 4 weeks). The primary outcome was placental malaria diagnosed by histopathology, placental blood smear, and/or placental blood loop-mediated isothermal amplification. Multivariate analyses were performed using logistic regression models. Subgroup analysis was performed based on the presence of symptomatic malaria, gravidity, and timing of infection.
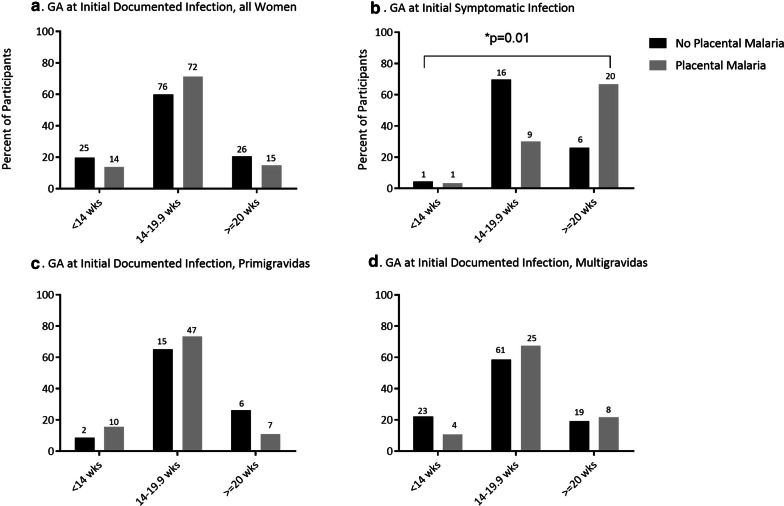
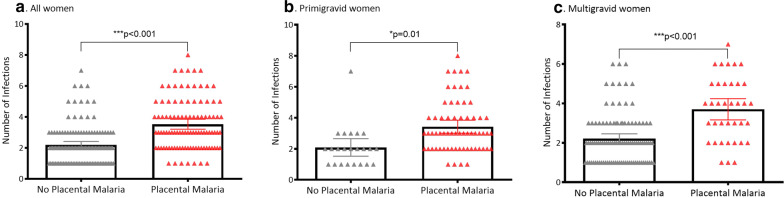
Results: Of the 228 patients with documented maternal infection with malaria parasites during pregnancy, 101 (44.3%) had placental malaria. Primigravidity was strongly associated with placental malaria (aOR 8.90, 95% CI 4.34-18.2, p < 0.001), and each episode of malaria was associated with over a twofold increase in placental malaria (aOR 2.35, 95% CI 1.69-3.26, p < 0.001). Among multigravid women, the odds of placental malaria increased by 14% with each advancing week of gestation at first documented infection (aOR 1.14, 95% CI 1.02-1.27, p = 0.02). When stratified by the presence of symptoms, primigravidity was only associated with placental malaria in asymptomatic women, who had a 12-fold increase in the odds of placental malaria (aOR 12.19, 95% CI 5.23-28.43, p < 0.001).
Conclusions: Total number of P. falciparum infections in pregnancy is a significant predictor of placental malaria. The importance of timing of infection on the development of placental malaria varies based on gravidity. In primigravidas, earlier asymptomatic infections were more frequently identified in those with placental malaria, whereas in multigravidas, parasitaemias detected later in gestation were associated with placental malaria. Earlier initiation of an effective intermittent preventive therapy may help to prevent placental malaria and improve birth outcomes, particularly in primigravid women.
Keywords: Africa; Global health; Infectious disease; Obstetrics; Perinatal outcome; Plasmodium falciparum; Pregnancy; Primigravid.
Conflict of interest statement
The authors report no conflict of interest.
Figures
References
-
- WHO. World malaria report 2019. https://www.who.int/news-room/feature-stories/detail/world-malaria-repor.... Accessed 27 May 2020
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
