

Longitudinal Auxological recovery in a cohort of children with Hyperinsulinaemic Hypoglycaemia
- PMID: 32580746
- PMCID: PMC7313198
- DOI: 10.1186/s13023-020-01438-0
Longitudinal Auxological recovery in a cohort of children with Hyperinsulinaemic Hypoglycaemia
Abstract
Background: Hypoglycaemia due to hyperinsulinism (HI) is the commonest cause of severe, recurrent hypoglycaemia in childhood. Cohort outcomes of HI remain to be described and whilst previous follow up studies have focused on neurodevelopmental outcomes, there is no information available on feeding and auxology.
Aim: We aimed to describe HI outcomes for auxology, medications, feeding and neurodevelopmental in a cohort up to age 5 years.
Method: We reviewed medical records for all patients with confirmed HI over a three-year period in a single centre to derive a longitudinal dataset.
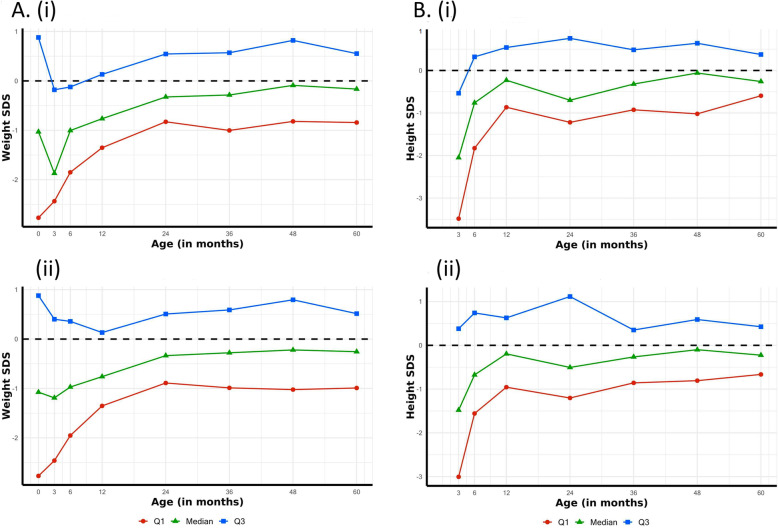
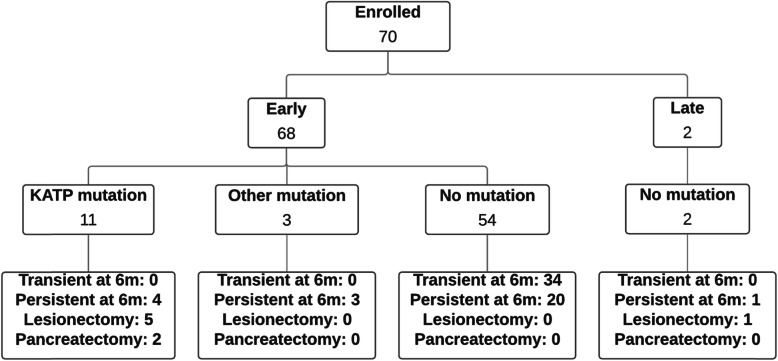
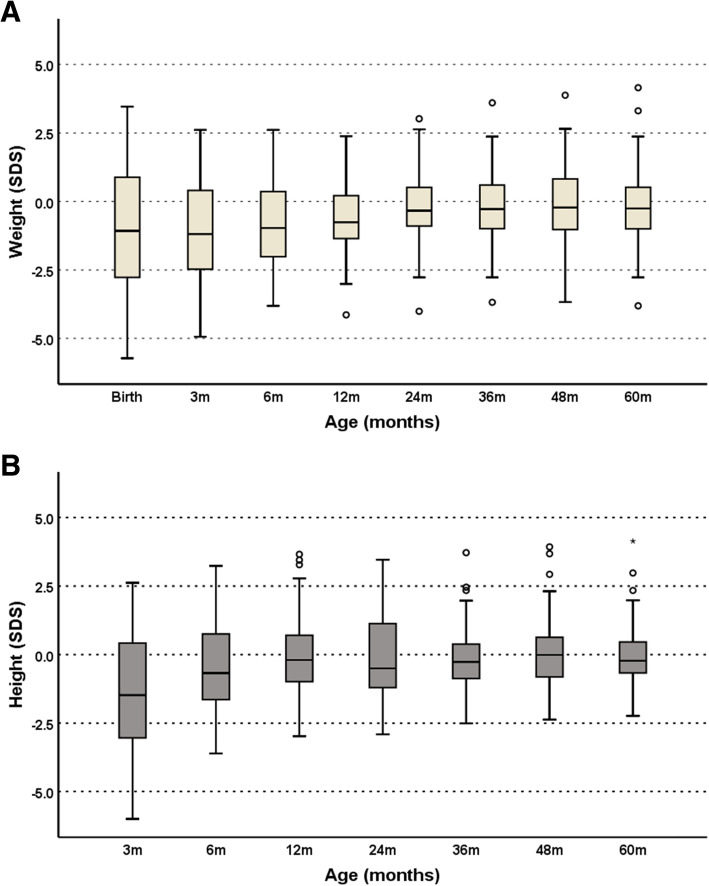
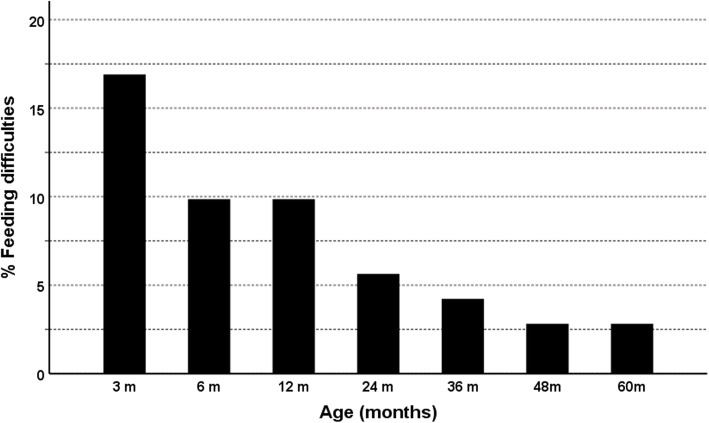
Results: Seventy patients were recruited to the study. Mean weight at birth was - 1.0 standard deviation scores (SDS) for age and sex, while mean height at 3 months was - 1.5 SDS. Both weight and height trended to the population median over the follow up period. Feeding difficulties were noted in 17% of patients at 3 months and this reduced to 3% by 5 years. At age 5 years, 11 patients (15%) had neurodevelopmental delay and of these only one was severe. Resolution of disease was predicted by lower maximum early diazoxide dose (p = 0.007) and being born SGA (p = 0.009).
Conclusion: In a three-year cohort of HI patients followed up for 5 years, in spite of feeding difficulties and carbohydrate loading in early life, auxology parameters are normal in follow up. A lower than expected rate of neurodevelopmental delay could be attributed to prompt early treatment.
Keywords: Congenital Hyperinsulinism; Diazoxide; Height; Hypoglycaemia; Natural history; Neurodevelopment; Outcomes; Weight.
Conflict of interest statement
None.
Figures

References
-
- Yau D, Laver TW, Dastamani A, Senniappan S, Houghton JAL, Shaikh G, et al. Using referral rates for genetic testing to determine the incidence of a rare disease: The minimal incidence of congenital hyperinsulinism in the UK is 1 in 28,389. Brusgaard K, editor. PLoS One. 2020;15(2):e0228417. doi: 10.1371/journal.pone.0228417. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
