

Genicular Nerve Pulsed Dose Radiofrequency (PDRF) Compared to Intra-Articular and Genicular Nerve PDRF in Knee Osteoarthritis Pain: A Propensity Score-Matched Analysis
- PMID: 32581573
- PMCID: PMC7280065
- DOI: 10.2147/JPR.S240138
Genicular Nerve Pulsed Dose Radiofrequency (PDRF) Compared to Intra-Articular and Genicular Nerve PDRF in Knee Osteoarthritis Pain: A Propensity Score-Matched Analysis
Abstract
Background: Chronic knee osteoarthritic (OA) pain is a common and debilitating complaint in elderly patients. Despite numerous pharmaceutical options, the majority of patients still experience long-term pain. Genicular nerve (GN) radiofrequency has become increasingly popular as a treatment for knee pain. This retrospective study aimed to evaluate the effects of pulse dose radiofrequency (PDRF) in patients with chronic knee OA pain.
Patients and methods: Propensity score matching analysis was performed in a retrospective cohort of 78 patients with moderate-severe knee OA pain unresponsive to conservative treatment who underwent PDRF GN or intra-articular (IA) and PDRF GN. Pain relief was measured using the numeric rating scale (NRS), Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) and Patient Global Impression of Change (PGIC) at 3 and 6 months post-intervention.
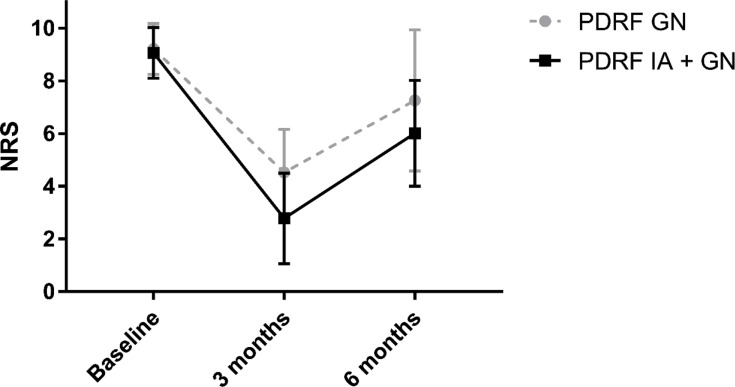
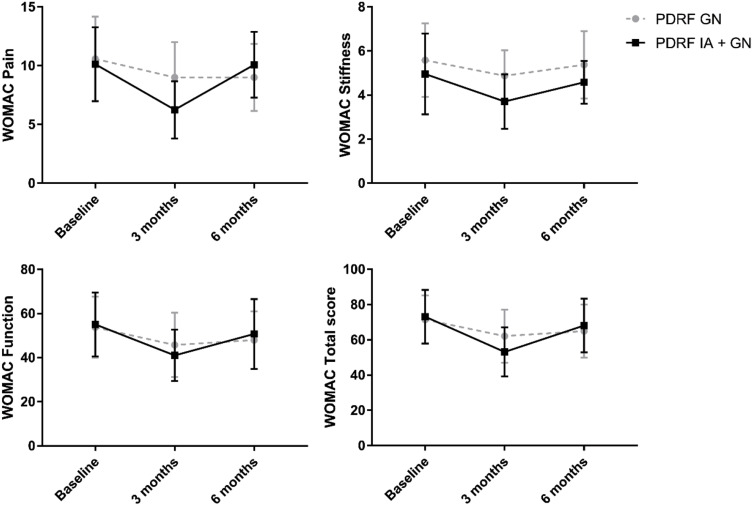
Results: A significant reduction in NRS scores was reported at 3 (p<0.001) and 6 months (p<0.001) after PDRF in both groups. NRS was lower in PDRF IA + GN than PDRF GN (p<0.0001). WOMAC pain was significantly reduced at 3 months in PDRF IA + GN group (baseline: 10.12±3.14, 3 months: 6.25±2.44, p=0.0001). WOMAC stiffness and function were improved only at 3 months in PDRF IA + GN compared to baseline (p=0.007 and p=0.006, respectively). A longer period of pain relief was reported after PDRF IA + GN (6.75±2.42 months) compared to PDRF GN (4.31±2.85 months, p<0.001) in association with higher PGIC scores.
Conclusion: This is the first study that compared two different PDRF techniques. PDRF GN and PDRF IA + GN were both effective in reducing pain at 3 and 6 months follow-up. However, only PDRF IA + GN was able to improve WOMAC scores at 3 months after the treatment with a longer period of efficacy compared to PDRF GN alone.
Keywords: WOMAC; chronic pain; interventional pain management; knee pain; osteoarthritis; pulse dose radiofrequency; PDRF; radiofrequency; genicular nerve.
© 2020 Leoni et al.
Conflict of interest statement
Dr Michael E Schatman reports consultancy for Kaleo Pharma, Salix Pharmaceuticals, and Quest Diagnostics, outside the submitted work. Drs Laura Demartini reports personal fees from Boston Scientific, personal fees from Abbott, personal fees from Grunenthal Italia, outside the submitted work. The authors report no other conflicts of interest in this work.
Figures
References
LinkOut - more resources
Full Text Sources
