

Combined Imhauser osteotomy and osteochondroplasty in slipped capital femoral epiphysis through surgical hip dislocation approach
- PMID: 32582386
- PMCID: PMC7302412
- DOI: 10.1302/1863-2548.14.200021
Combined Imhauser osteotomy and osteochondroplasty in slipped capital femoral epiphysis through surgical hip dislocation approach
Abstract
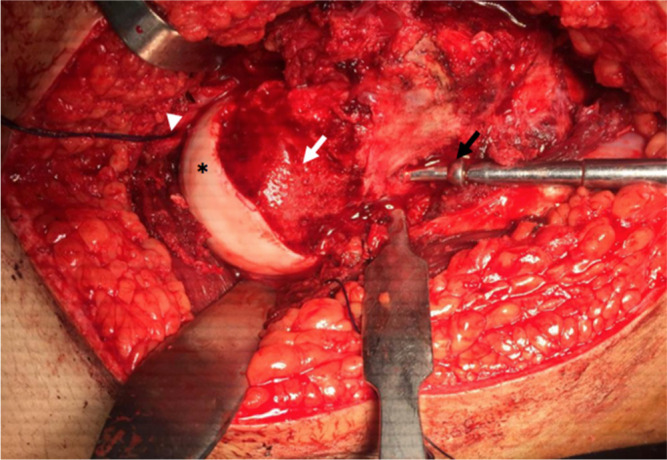
Purpose: Treatment of moderate to severe stable slipped capital femoral epiphysis (SCFE) remains a challenging problem. Open reduction by modified Dunn procedure carries a considerable risk of osteonecrosis (ON). Imhauser osteotomy is capable of realigning the deformity without the risk of ON, but the remaining metaphyseal bump is implicated with significant chondro-labral lesions and accelerated osteoarthritis. We conducted this study to evaluate the efficacy and safety of Imhauser osteotomy combined with osteochondroplasty (OCP) through the surgical hip dislocation (SHD) approach.
Methods: A prospective series of 23 patients with moderate-severe stable SCFE underwent Imhauser osteotomy and OCP through SHD. The mean age was 14.4 years (13 to 20) and the mean follow-up period was 45 months (24 to 66). The outcome measures included clinical and radiological parameters and Harris hip score (HHS) was used as a functional score.
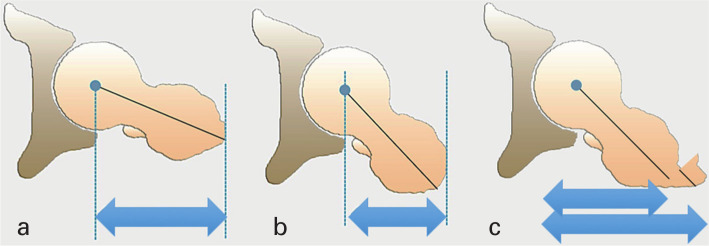
Results: The mean HHS improved significantly from 65.39 to 93.3. The limb length discrepancy improved by a mean of 1.72 cm. The mean flexion and abduction arcs showed a significant improvement (mean increase of 37.5° and 18.5°, respectively). The mean internal rotation demonstrated the most significant improvement (mean increase of 38.5°). All the radiographic parameters improved significantly; including anterior and lateral slip angles (mean improvement 37.52° and 44.37°, respectively). The mean alpha angle decreased by 39.19°. The articulo-trochanteric distance significantly increased to a mean of 23.26 mm. No cases of ON or chondrolysis were identified.
Conclusion: Combined Imhauser osteotomy and OCP through the surgical dislocation approach provide a comprehensive and safe management of moderate to severe stable SCFE.
Level of evidence: IV.
Keywords: Imhauser osteotomy; hip impingement; hip preservation; slipped capital femoral epiphysis; surgical hip dislocation.
Copyright © 2020, The author(s).
Figures




References
-
- Aronsson DD, Loder RT. Treatment of the unstable (acute) slipped capital femoral epiphysis. Clin Orthop Relat Res 1996;322:99-110. - PubMed
-
- Castañeda P, Ponce C, Villareal G, Vidal C. The natural history of osteoarthritis after a slipped capital femoral epiphysis / the pistol grip deformity. J Pediatr Orthop 2013;33:S76-S82. - PubMed
-
- Sink EL, Zaltz I, Heare T, Dayton M. Acetabular cartilage and labral damage observed during surgical hip dislocation for stable slipped capital femoral epiphysis. J Pediatr Orthop 2010;30:26-30. - PubMed
-
- Ganz R, Parvizi J, Beck M, et al. Femoroacetabular impingement: a cause for osteoarthritis of the hip. Clin Orthop Relat Res 2003;417:112-120. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
