

T-Cell Replete Myeloablative Haploidentical Bone Marrow Transplantation Is an Effective Option for Pediatric and Young Adult Patients With High-Risk Hematologic Malignancies
- PMID: 32582591
- PMCID: PMC7295947
- DOI: 10.3389/fped.2020.00282
T-Cell Replete Myeloablative Haploidentical Bone Marrow Transplantation Is an Effective Option for Pediatric and Young Adult Patients With High-Risk Hematologic Malignancies
Abstract
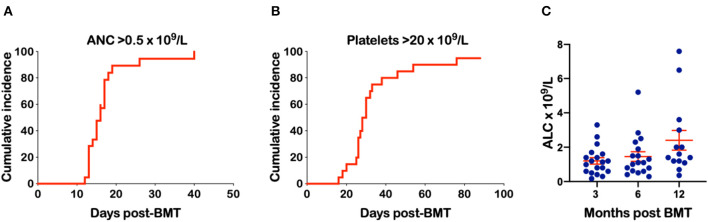
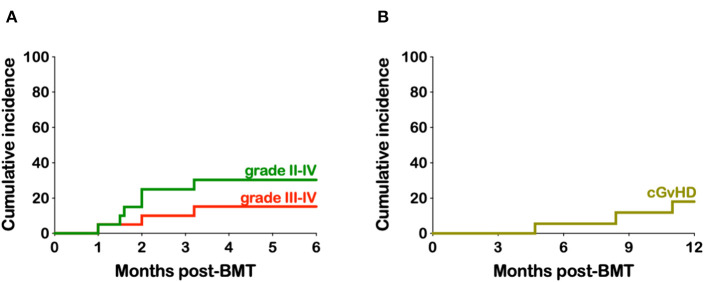
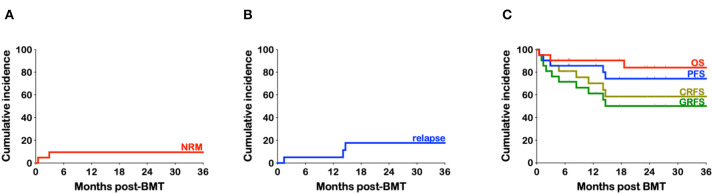
Twenty-one pediatric and young adult patients (1.1-24.7 years) with hematologic malignancies underwent myeloablative T-cell replete haploidentical bone marrow transplant (haplo-BMT) between October 2015 to December 2019. Fifty-seven percent of the patients were ethnic or racial minorities. Thirteen patients had B-cell precursor acute lymphoblastic leukemia (B-ALL) with 10 receiving 1,200 cGy fractionated total body irradiation with fludarabine while the remaining 11 patients had targeted dose-busulfan, fludarabine, melphalan conditioning. Graft-vs.-host disease (GvHD) prophylaxis consisted of post-transplant cyclophosphamide (15 patients) or cyclophosphamide and bendamustine (six patients), with all patients receiving tacrolimus and mycophenolate mofetil. Twelve patients were in first or second remission at time of transplant with five in >2nd remission and four with measurable disease. Three patients had failed prior transplants and three CAR-T cell therapies. Only one patient developed primary graft failure but engrafted promptly after a second conditioned T-replete peripheral blood stem cell transplant from the same donor. An absolute neutrophil count of 0.5 × 109/L was achieved at a median time of 16 days post-BMT while platelet engraftment occurred at a median of 30 days. The cumulative incidence of grades III to IV acute GvHD and chronic GvHD was 15.2 and 18.1%, respectively. With a median follow-up of 25.1 months the relapse rate is 17.6% with an overall survival of 84.0% and a progression-free survival of 74.3%. The chronic graft-vs.-host-free relapse-free survival (CRFS) is 58.5% while acute and chronic graft-vs.-host-free relapse-free survival (GRFS) is 50.1%. Myeloablative conditioned T-replete haploidentical BMT is a viable alternative to matched unrelated transplantation for children and young adults with high-risk hematologic malignancies.
Keywords: GvHD; T-replete; haploidentical BMT; myeloablative; pediatric.
Copyright © 2020 Katsanis, Sapp, Reid, Reddivalla and Stea.
Figures
References
-
- Luznik L, O'Donnell PV, Symons HJ, Chen AR, Leffell MS, Zahurak M, et al. HLA-haploidentical bone marrow transplantation for hematologic malignancies using nonmyeloablative conditioning and high-dose, posttransplantation cyclophosphamide. Biol Blood Marrow Transplant. (2008) 14:641–50. 10.1016/j.bbmt.2008.03.005 - DOI - PMC - PubMed
-
- Bacigalupo A, Dominietto A, Ghiso A, Di Grazia C, Lamparelli T, Gualandi F, et al. Unmanipulated haploidentical bone marrow transplantation and post-transplant cyclophosphamide for hematologic malignanices following a myeloablative conditioning: an update. Bone Marrow Transplant. (2015) 50 (Suppl. 2):S37–9. 10.1038/bmt.2015.93 - DOI - PubMed
-
- Bashey A, Zhang X, Jackson K, Brown S, Ridgeway M, Solh M, et al. Comparison of outcomes of hematopoietic cell transplants from T-replete haploidentical donors using post-transplantation cyclophosphamide with 10 of 10 HLA-A, -B, -C, -DRB1, and -DQB1 allele-matched unrelated donors and HLA-identical sibling donors: a multivariable analysis including disease risk index. Biol Blood Marrow Transplant. (2016) 22:125–33. 10.1016/j.bbmt.2015.09.002 - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Medical