

Characterization of Human Colon Organoids From Inflammatory Bowel Disease Patients
- PMID: 32582690
- PMCID: PMC7287042
- DOI: 10.3389/fcell.2020.00363
Characterization of Human Colon Organoids From Inflammatory Bowel Disease Patients
Abstract
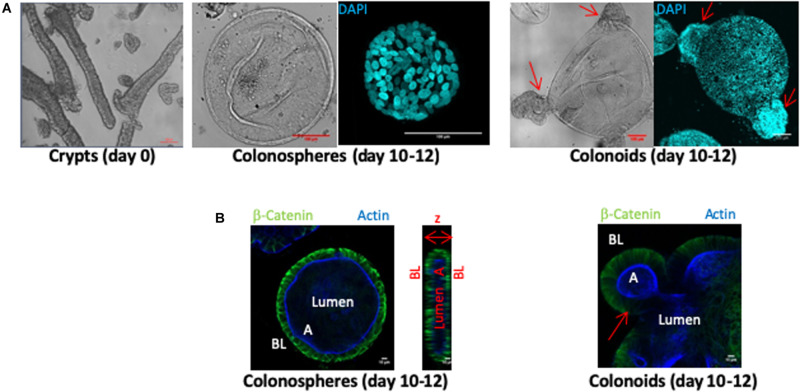
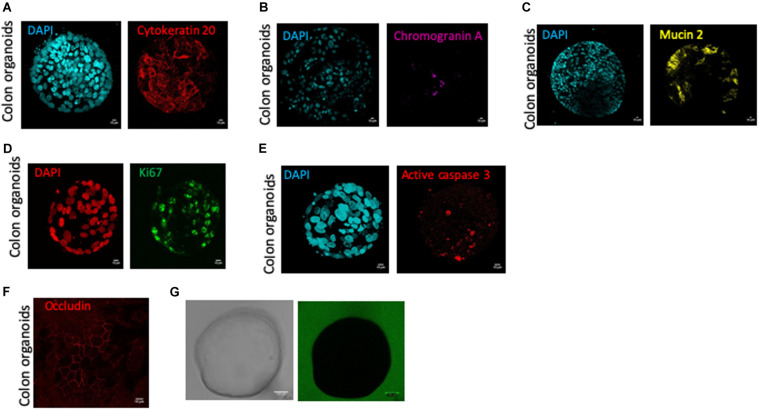
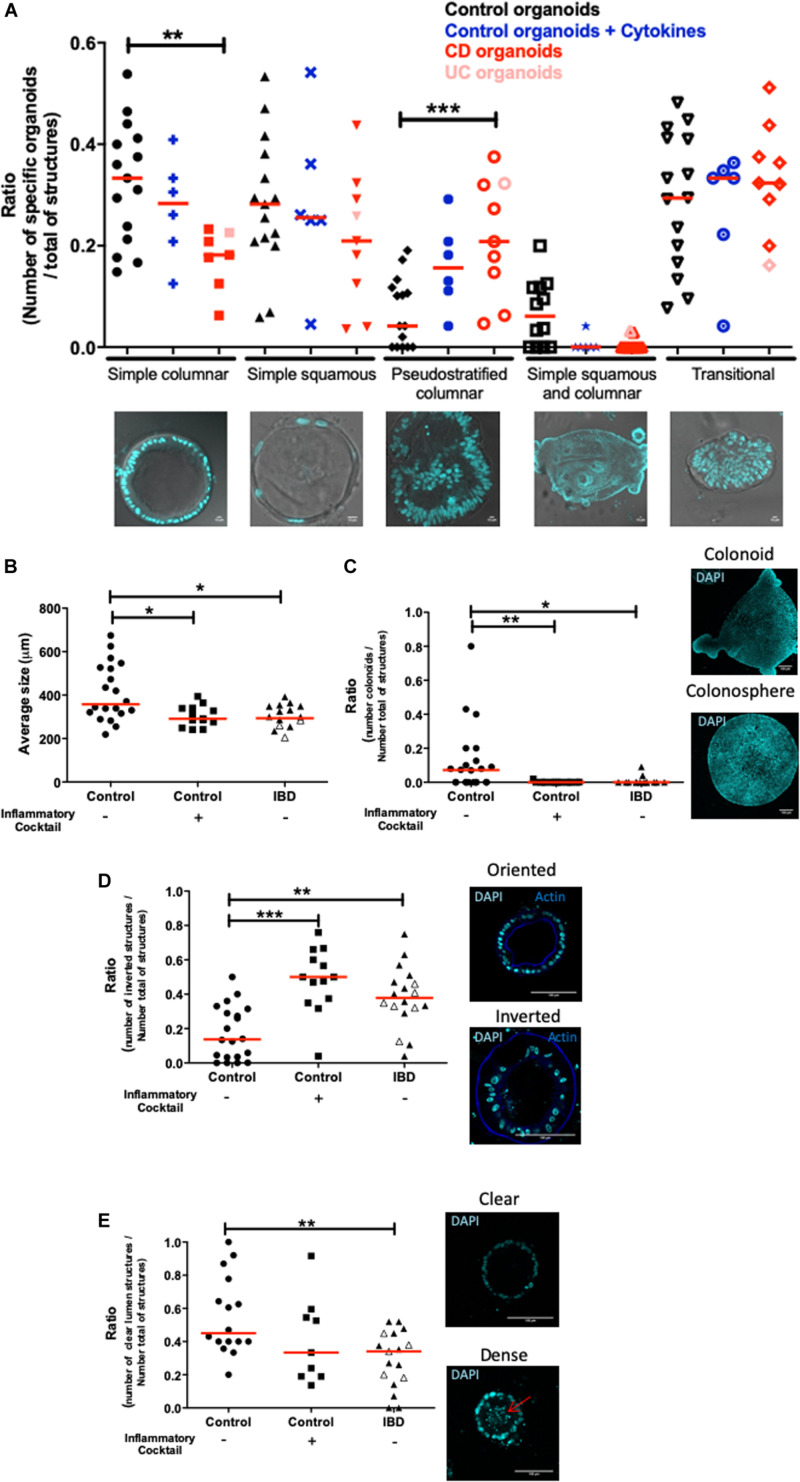
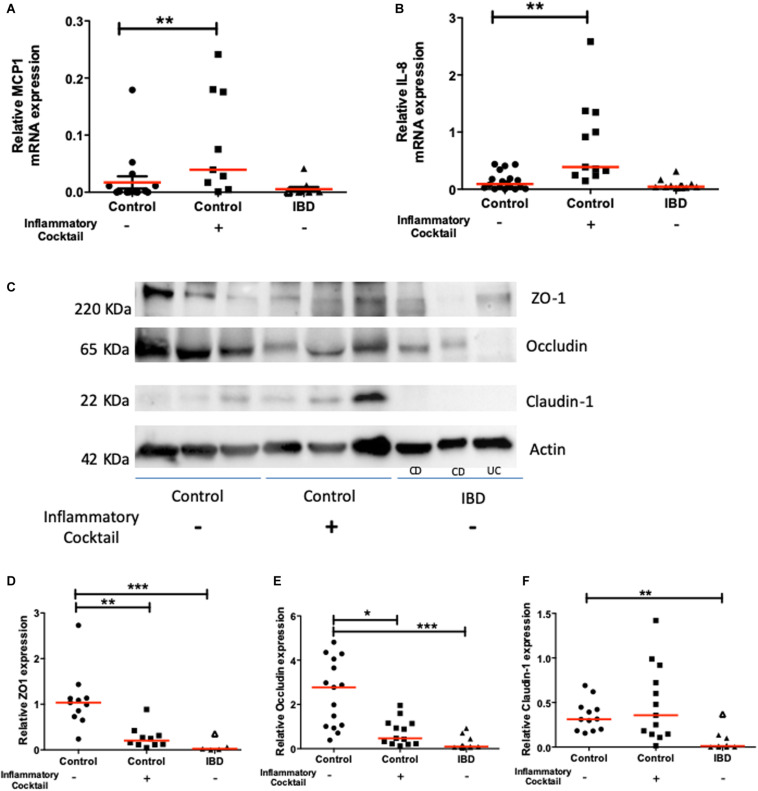
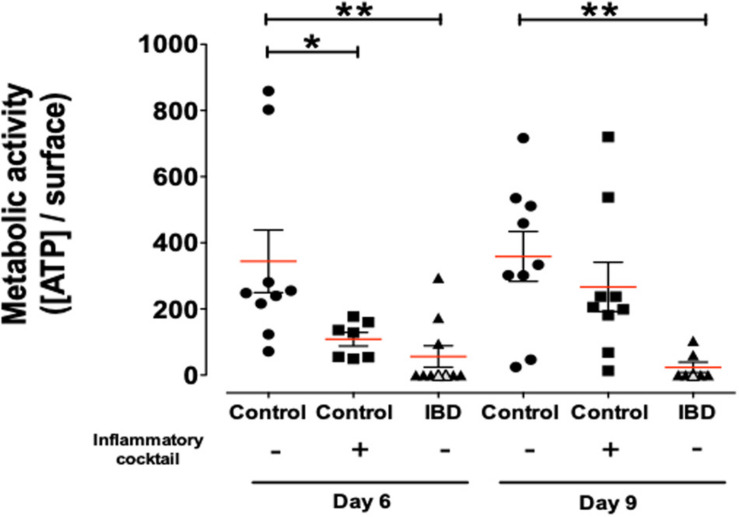
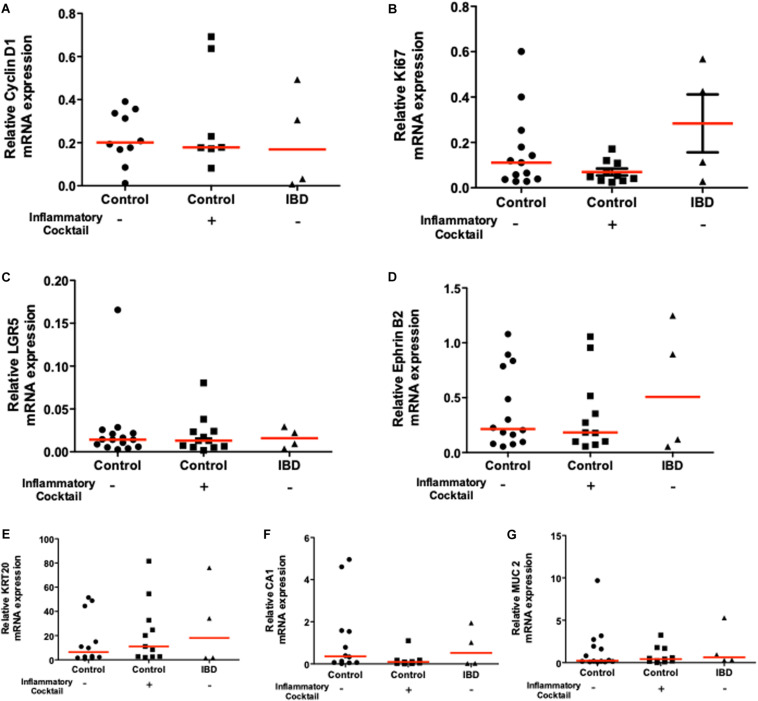
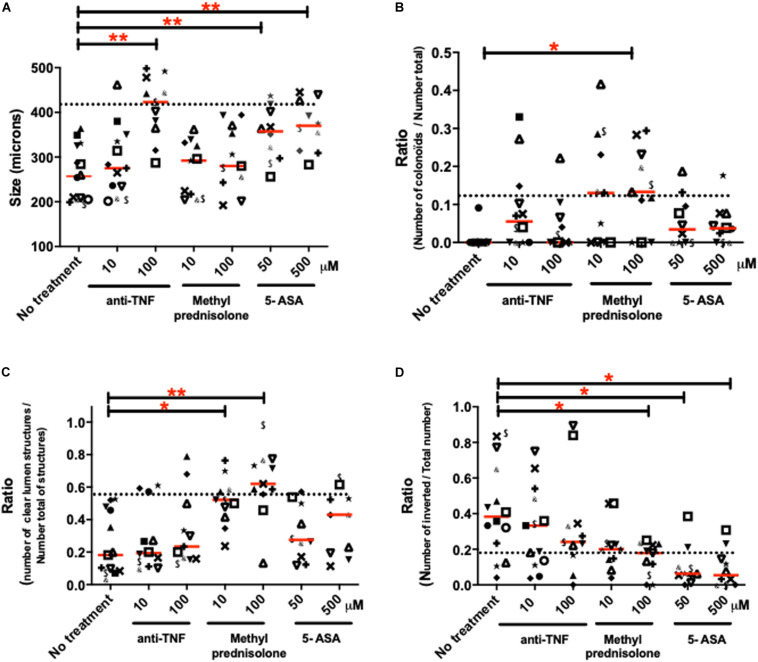
Inflammatory Bowel Diseases (IBD) are chronic inflammatory disorders, where epithelial defects drive, at least in part, some of the pathology. We reconstituted human intestinal epithelial organ, by using three-dimension culture of human colon organoids. Our aim was to characterize morphological and functional phenotypes of control (non-IBD) organoids, compared to inflamed organoids from IBD patients. The results generated describe the epithelial defects associated with IBD in primary organoid cultures, and evaluate the use of this model for pharmacological testing of anti-inflammatory approaches. Human colonic tissues were obtained from either surgical resections or biopsies, all harvested in non-inflammatory zones. Crypts were isolated from controls (non-IBD) and IBD patients and were cultured up to 12-days. Morphological (size, budding formation, polarization, luminal content), cell composition (proliferation, differentiation, immaturity markers expression), and functional (chemokine and tight junction protein expression) parameters were measured by immunohistochemistry, RT-qPCR or western-blot. The effects of inflammatory cocktail or anti-inflammatory treatments were studied in controls and IBD organoid cultures respectively. Organoid cultures from controls or IBD patients had the same cell composition after 10 to 12-days of culture, but IBD organoid cultures showed an inflammatory phenotype with decreased size and budding capacity, increased cell death, luminal debris, and inverted polarization. Tight junction proteins were also significantly decreased in IBD organoid cultures. Inflammatory cytokine cocktail reproduced this inflammatory phenotype in non-IBD organoids. Clinically used treatments (5-ASA, glucocorticoids, anti-TNF) reduced some, but not all parameters. Inflammatory phenotype is associated with IBD epithelium, and can be studied in organoid cultures. This model constitutes a reliable human pre-clinical model to investigate new strategies targeting epithelial repair.
Keywords: Crohn’s disease; inflammation; intestine; organoid; ulcerative colitis.
Copyright © 2020 d’Aldebert, Quaranta, Sébert, Bonnet, Kirzin, Portier, Duffas, Chabot, Lluel, Allart, Ferrand, Alric, Racaud-Sultan, Mas, Deraison and Vergnolle.
Figures
References
-
- Panaccione R., Ferraz J. G., Beck P. (2005). Advances in medical therapy of inflammatory bowel disease. Curr.Opin.Pharmacol. 5 566–572. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources