

Lung Cancer Screening with Low-Dose CT: a Meta-Analysis
- PMID: 32583338
- PMCID: PMC7573097
- DOI: 10.1007/s11606-020-05951-7
Lung Cancer Screening with Low-Dose CT: a Meta-Analysis
Abstract
Background: Randomized controlled trials have evaluated the efficacy of low-dose CT (LDCT) lung cancer screening on lung cancer (LC) outcomes.
Objective: Meta-analyze LDCT lung cancer screening trials.
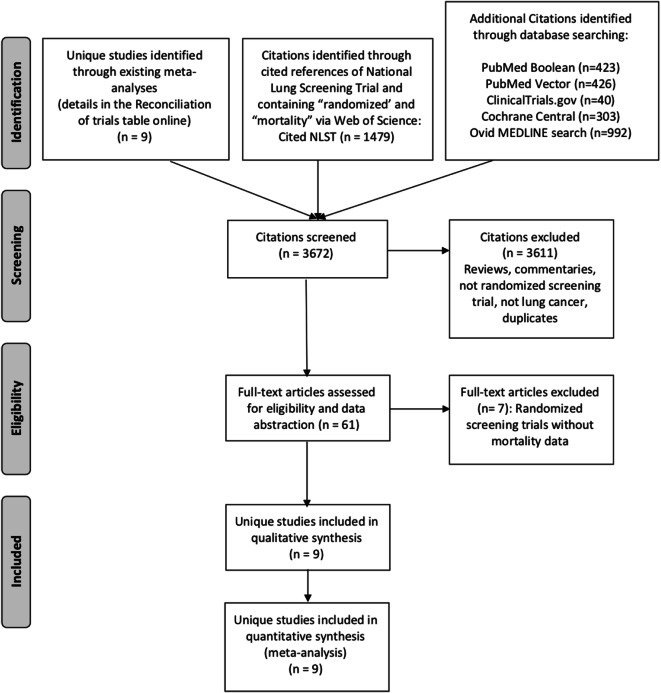
Methods: We identified studies by searching PubMed, Google Scholar, the Cochrane Registry, ClinicalTrials.gov , and reference lists from retrieved publications. We abstracted data on study design features, stage I LC diagnoses, LC and overall mortality, false positive results, harm from invasive diagnostic procedures, overdiagnosis, and significant incidental findings. We assessed study quality using the Cochrane risk-of-bias tool. We used random-effects models to calculate relative risks and assessed effect modulators with subgroup analyses and meta-regression.
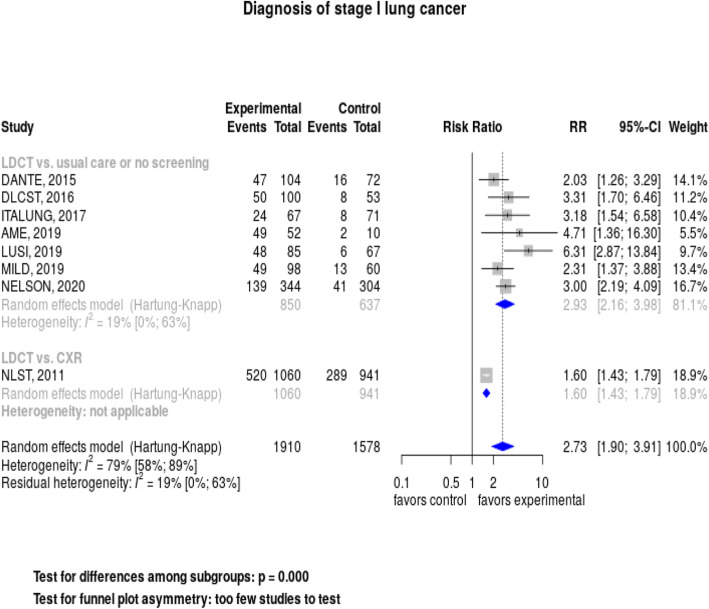
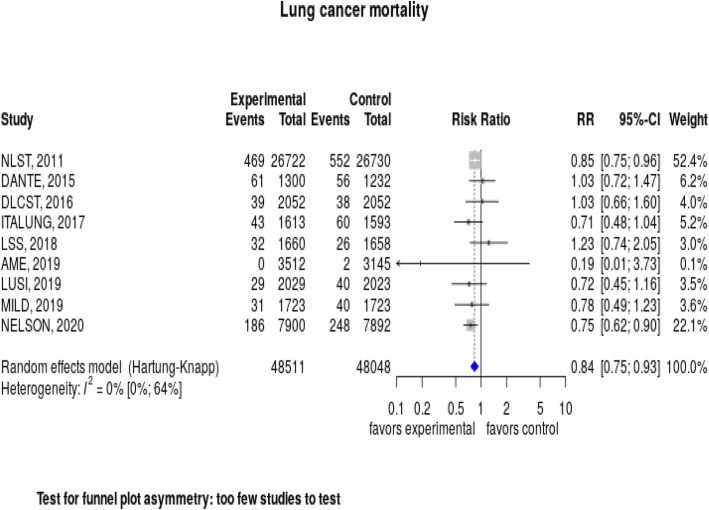
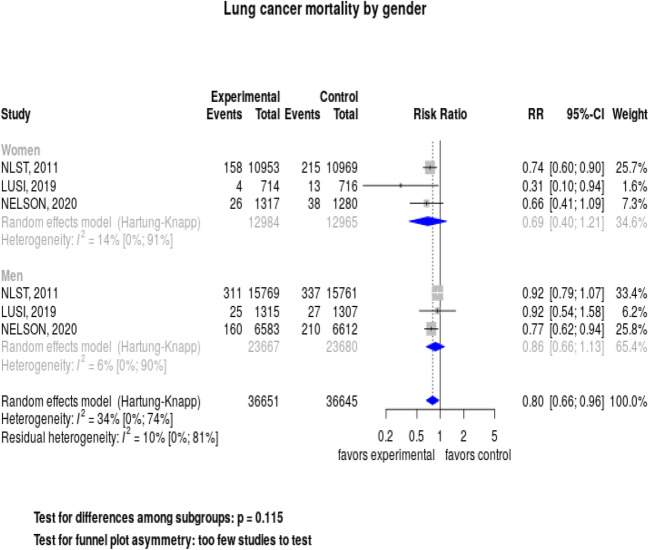
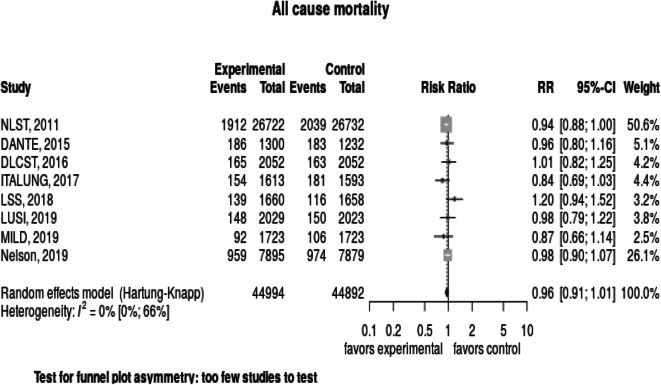
Results: We identified 9 studies that enrolled 96,559 subjects. The risk of bias across studies was judged to be low. Overall, LDCT screening significantly increased the detection of stage I LC, RR = 2.93 (95% CI, 2.16-3.98), I2 = 19%, and reduced LC mortality, RR = 0.84 (95% CI, 0.75-0.93), I2 = 0%. The number needed to screen to prevent an LC death was 265. Women had a lower risk of LC death (RR = 0.69, 95% CI, 0.40-1.21) than men (RR = 0.86, 95% CI, 0.66-1.13), p value for interaction = 0.11. LDCT screening did not reduce overall mortality, RR = 0.96 (95% CI, 0.91-1.01), I2 = 0%. The pooled false positive rate was 8% (95% CI, 4-18); subjects with false positive results had < 1 in 1000 risk of major complications following invasive diagnostic procedures. The most valid estimates for overdiagnosis and significant incidental findings were 8.9% and 7.5%, respectively.
Discussion: LDCT screening significantly reduced LC mortality, though not overall mortality, with women appearing to benefit more than men. The estimated risks for false positive results, screening complications, overdiagnosis, and incidental findings were low. Long-term survival data were available only for North American and European studies limiting generalizability.
Keywords: low-dose computed tomography; lung cancer screening; lung neoplasms; meta-analysis; mortality.
Conflict of interest statement
The authors declare that they do not have a conflict of interest.
Figures
References
-
- Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68:394–424. - PubMed
-
- US Department of Health and Human Services. The health consequences of smoking: 50 years of progress. A report of the Surgeon General. Atlanta, GA: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, Natonal Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health; 2014.
-
- de Koning HJ, van der Aalst CM, de Jong PA, et al. Reduced Lung-Cancer Mortality with Volume CT Screening in a Randomized Trial. N Engl J Med. 2020;382:503–13. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
