

A deep learning framework for prostate localization in cone beam CT-guided radiotherapy
- PMID: 32583418
- PMCID: PMC10823910
- DOI: 10.1002/mp.14355
A deep learning framework for prostate localization in cone beam CT-guided radiotherapy
Abstract
Purpose: To develop a deep learning-based model for prostate planning target volume (PTV) localization on cone beam computed tomography (CBCT) to improve the workflow of CBCT-guided patient setup.
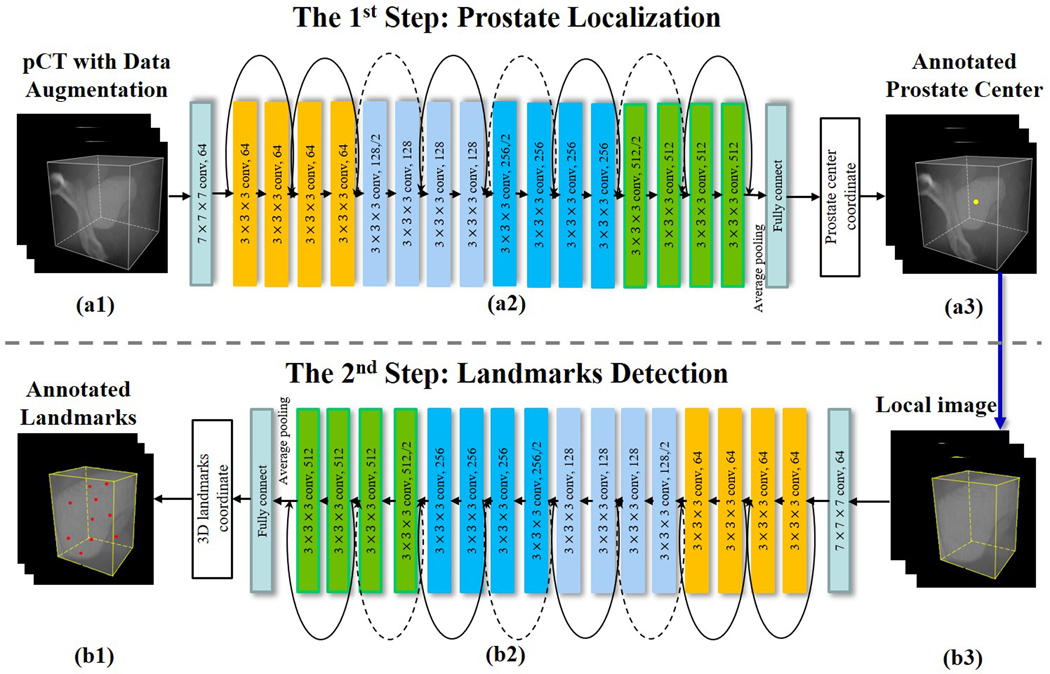
Methods: A two-step task-based residual network (T2 RN) is proposed to automatically identify inherent landmarks in prostate PTV. The input to the T2 RN is the pretreatment CBCT images of the patient, and the output is the deep learning-identified landmarks in the PTV. To ensure robust PTV localization, the T2 RN model is trained by using over thousand sets of CT images with labeled landmarks, each of the CTs corresponds to a different scenario of patient position and/or anatomy distribution generated by synthetically changing the planning CT (pCT) image. The changes, including translation, rotation, and deformation, represent vast possible clinical situations of anatomy variations during a course of radiation therapy (RT). The trained patient-specific T2 RN model is tested by using 240 CBCTs from six patients. The testing CBCTs consists of 120 original CBCTs and 120 synthetic CBCTs. The synthetic CBCTs are generated by applying rotation/translation transformations to each of the original CBCT.
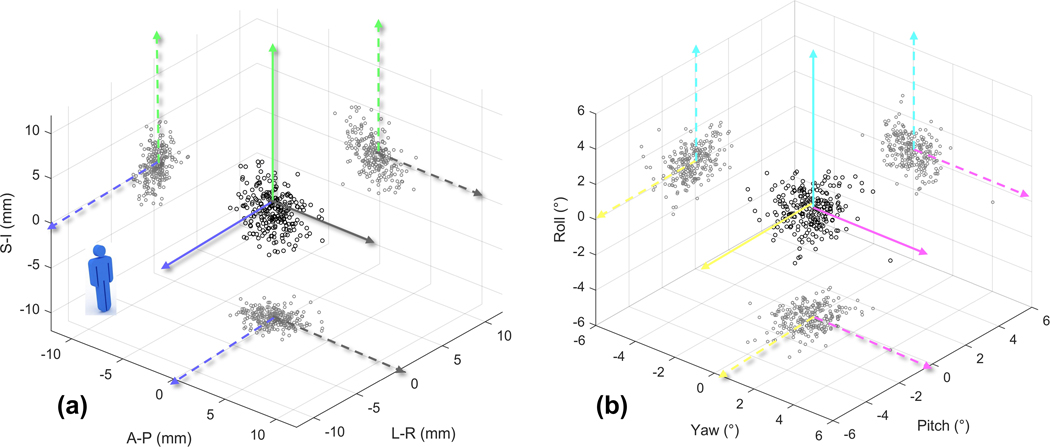
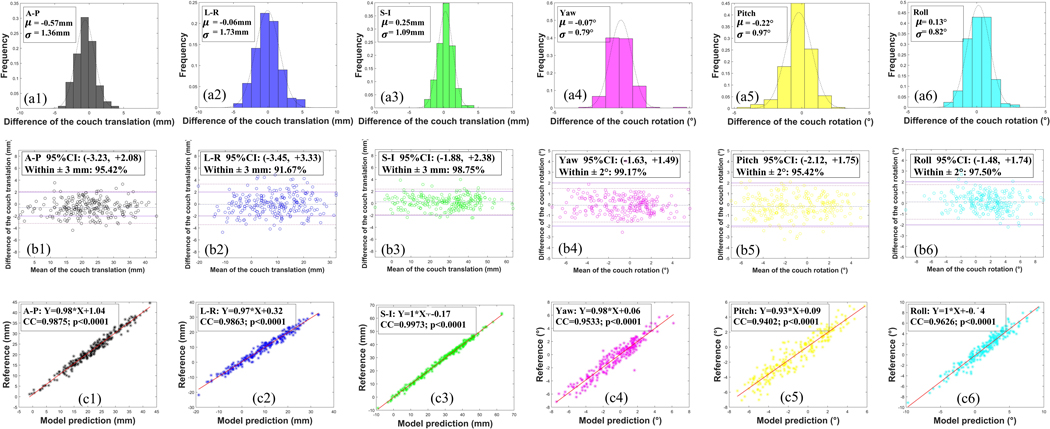
Results: The systematic/random setup errors between the model prediction and the reference are found to be <0.25/2.46 mm and 0.14/1.41° in translation and rotation dimensions, respectively. Pearson's correlation coefficient between model prediction and the reference is higher than 0.94 in translation and rotation dimensions. The Bland-Altman plots show good agreement between the two techniques.
Conclusions: A novel T2 RN deep learning technique is established to localize the prostate PTV for RT patient setup. Our results show that highly accurate marker-less prostate setup is achievable by leveraging the state-of-the-art deep learning strategy.
Keywords: CBCT; IGRT; deep learning; localization; prostate; radiotherapy.
© 2020 American Association of Physicists in Medicine.
Figures
References
-
- Marchant TE, Amer AM, Moore CJ, “Measurement of inter and intra fraction organ motion in radiotherapy using cone beam CT projection images,” Physics in Medicine & Biology 53, 1087 (2008). - PubMed
-
- Kadoya N, Cho SY, Kanai T, Onozato Y, Ito K, Dobashi S, Yamamoto T, Umezawa R, Matsushita H, Takeda K, “Dosimetric impact of 4-dimensional computed tomography ventilation imaging-based functional treatment planning for stereotactic body radiation therapy with 3-dimensional conformal radiation therapy,” Practical radiation oncology 5, e505–e512 (2015). - PubMed
-
- Kupelian PA, Langen KM, Willoughby TR, Zeidan OA, Meeks SL, “Image-guided radiotherapy for localized prostate cancer: treating a moving target,” Semin Radiat Oncol 18, 58–66 (2008). - PubMed
-
- Kupelian PA, Lee C, Langen KM, Zeidan OA, Manon RR, Willoughby TR, Meeks SL, “Evaluation of image-guidance strategies in the treatment of localized prostate cancer,” Int J Radiat Oncol Biol Phys 70, 1151–1157 (2008). - PubMed
-
- Hargrave C, Deegan T, Poulsen M, Bednarz T, Harden F, Mengersen K, “A feature alignment score for online cone-beam CT-based image-guided radiotherapy for prostate cancer,” Med. Phys. 45, 2898–2911 (2018). - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
