

An Innovative Individual-Level Socioeconomic Measure Predicts Critical Care Outcomes in Older Adults: A Population-Based Study
- PMID: 32583721
- PMCID: PMC7759584
- DOI: 10.1177/0885066620931020
An Innovative Individual-Level Socioeconomic Measure Predicts Critical Care Outcomes in Older Adults: A Population-Based Study
Abstract
Background: Little is known about the impact of socioeconomic status (SES) as a key element of social determinants of health on intensive care unit (ICU) outcomes for adults.
Objective: We assessed whether a validated individual SES index termed HOUSES (HOUsing-based SocioEconomic status index) derived from housing features was associated with short-term outcomes of critical illness including ICU mortality, ICU-free days, hospital-free days, and ICU readmission.
Methods: We performed a population-based cohort study of adult patients living in Olmsted County, Minnesota, admitted to 7 intensive care units at Mayo Clinic from 2011 to 2014. We compared outcomes between the lowest SES group (HOUSES quartile 1 [Q1]) and the higher SES group (HOUSES Q2-4). We stratified the cohort based on age (<50 years old and ≥50 years old).
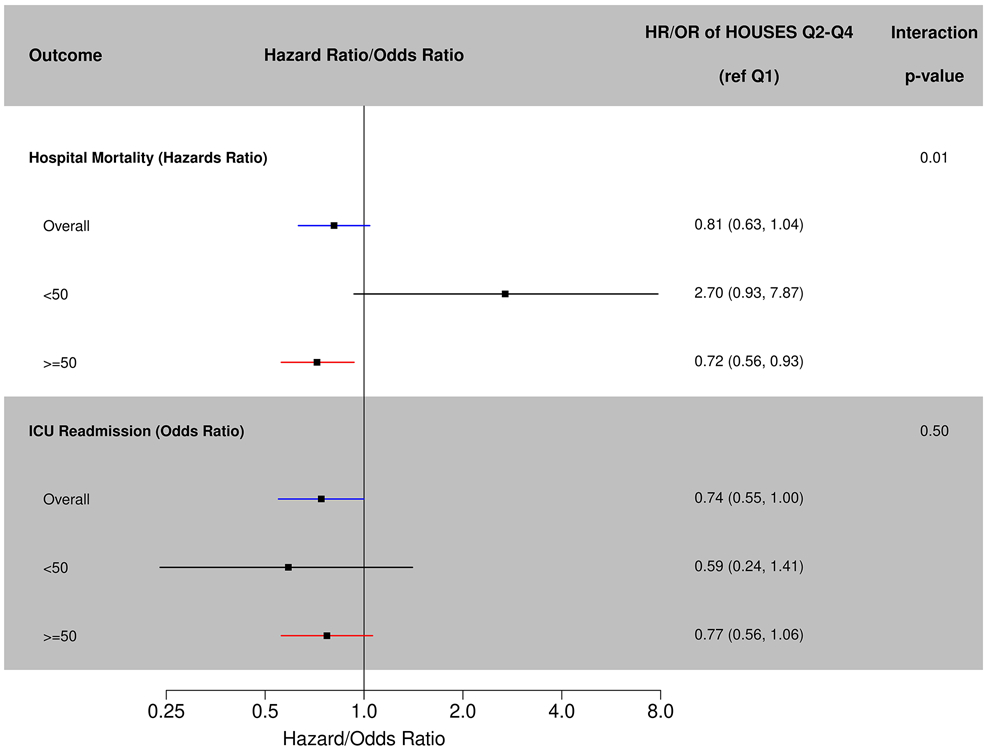
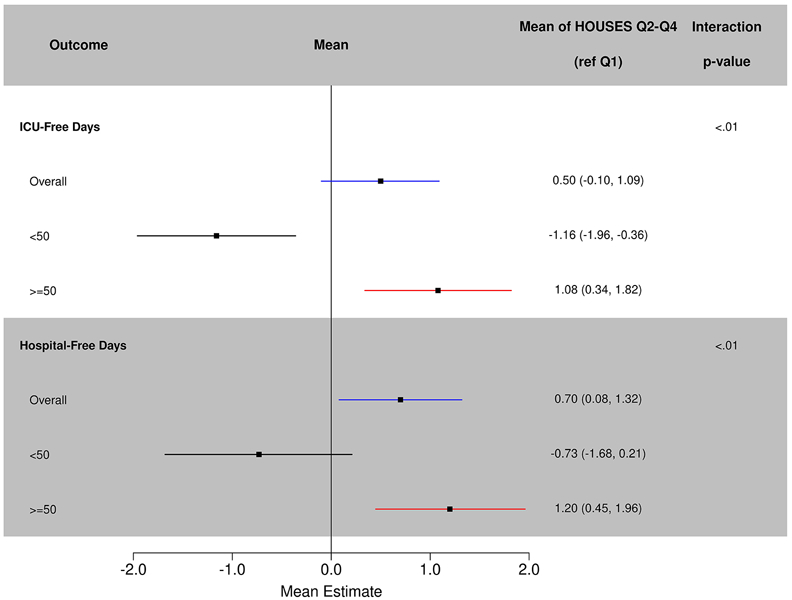
Results: Among 4134 eligible patients, 3378 (82%) patients had SES successfully measured by the HOUSES index. Baseline characteristics, severity of illness, and reason for ICU admission were similar among the different SES groups as measured by HOUSES except for larger number of intoxications and overdoses in younger patients from the lowest SES. In all adult patients, there were no overall differences in mortality, ICU-free days, hospital-free days, or ICU readmissions in patients with higher SES compared to lower SES. Among older patients (>50 years), those with higher SES (HOUSES Q2-4) compared to those with lower SES (HOUSES Q1) had lower mortality rates (hazard ratio = 0.72; 95% CI: 0.56-0.93; adjusted P = .01), increased ICU-free days (mean 1.08 days; 95% CI: 0.34-1.84; adjusted P = .004), and increased hospital-free days (mean 1.20 days; 95% CI: 0.45-1.96; adjusted P = .002). There were no differences in ICU readmission rates (OR = 0.74; 95% CI: 0.55-1.00; P = .051).
Conclusion: Individual-level SES may be an important determinant or predictor of critical care outcomes in older adults. Housing-based socioeconomic status may be a useful tool for enhancing critical care research and practice.
Keywords: ICU outcomes; Socioeconomic status; critical care; critical illness; length of stay; social determinants of health.
Conflict of interest statement
The authors have not disclosed any potential conflicts of interest.
Figures
Similar articles
-
An Individual Housing-Based Socioeconomic Status Measure Predicts Advance Care Planning and Nursing Home Utilization.Am J Hosp Palliat Care. 2019 May;36(5):362-369. doi: 10.1177/1049909118812431. Epub 2018 Nov 20. Am J Hosp Palliat Care. 2019. PMID: 30458635 Free PMC article.
-
A novel housing-based socioeconomic measure predicts hospitalisation and multiple chronic conditions in a community population.J Epidemiol Community Health. 2016 Mar;70(3):286-91. doi: 10.1136/jech-2015-205925. Epub 2015 Oct 12. J Epidemiol Community Health. 2016. PMID: 26458399 Free PMC article.
-
A novel measure of socioeconomic status using individual housing data to assess the association of SES with rheumatoid arthritis and its mortality: a population-based case-control study.BMJ Open. 2015 Apr 29;5(4):e006469. doi: 10.1136/bmjopen-2014-006469. BMJ Open. 2015. PMID: 25926142 Free PMC article.
-
HOUSES Index as an Innovative Socioeconomic Measure Predicts Graft Failure Among Kidney Transplant Recipients.Transplantation. 2020 Nov;104(11):2383-2392. doi: 10.1097/TP.0000000000003131. Transplantation. 2020. PMID: 31985729 Free PMC article.
-
The association between socioeconomic status and pandemic influenza: Systematic review and meta-analysis.PLoS One. 2021 Sep 7;16(9):e0244346. doi: 10.1371/journal.pone.0244346. eCollection 2021. PLoS One. 2021. PMID: 34492018 Free PMC article.
Cited by
-
Neighborhood Socioeconomic Disadvantage and Disability After Critical Illness.Crit Care Med. 2022 May 1;50(5):733-741. doi: 10.1097/CCM.0000000000005364. Epub 2021 Oct 12. Crit Care Med. 2022. PMID: 34636807 Free PMC article.
-
Association of Perinatal Factors With Severe Obesity and Dyslipidemia in Adulthood.J Prim Care Community Health. 2022 Jan-Dec;13:21501327211058982. doi: 10.1177/21501327211058982. J Prim Care Community Health. 2022. PMID: 35249418 Free PMC article.
-
Role of geographic risk factors and social determinants of health in COVID-19 epidemiology: Longitudinal geospatial analysis in a midwest rural region.J Clin Transl Sci. 2021 Dec 27;6(1):e51. doi: 10.1017/cts.2021.885. eCollection 2022. J Clin Transl Sci. 2021. PMID: 35651962 Free PMC article.
-
An Exploratory Analysis of Sociodemographic Factors Associated With Physical Functional Impairment in ICU Survivors.Crit Care Explor. 2024 Jun 5;6(6):e1100. doi: 10.1097/CCE.0000000000001100. eCollection 2024 Jun 1. Crit Care Explor. 2024. PMID: 38836576 Free PMC article.
-
Integrating Social Determinants of Health in Critical Care.CHEST Crit Care. 2024 Jun;2(2):100057. doi: 10.1016/j.chstcc.2024.100057. Epub 2024 Feb 19. CHEST Crit Care. 2024. PMID: 39238802 Free PMC article.
References
-
- Barrett ML, Smith MW, Elixhauser A, Honigman LS, Pines JM. STATISTICAL BRIEF# 185. 2014.
-
- Coopersmith CM, Wunsch H, Fink MP, et al. A comparison of critical care research funding and the financial burden of critical illness in the United States. Critical care medicine. 2012;40(4):1072–1079. - PubMed
-
- Halpern NA. Can the costs of critical care be controlled? Current opinion in critical care. 2009;15(6):591–596. - PubMed
-
- Mullins PM, Goyal M, Pines JM. National growth in intensive care unit admissions from emergency departments in the United States from 2002 to 2009. Academic Emergency Medicine. 2013;20(5):479–486. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
