

Efficacy and the Adverse Effects of Oral Versus Intravenous Arsenic for Acute Promyelocytic Leukemia: A Meta-Analysis of Randomized-Controlled Studies
- PMID: 32583728
- PMCID: PMC7318817
- DOI: 10.1177/1533033820937008
Efficacy and the Adverse Effects of Oral Versus Intravenous Arsenic for Acute Promyelocytic Leukemia: A Meta-Analysis of Randomized-Controlled Studies
Abstract
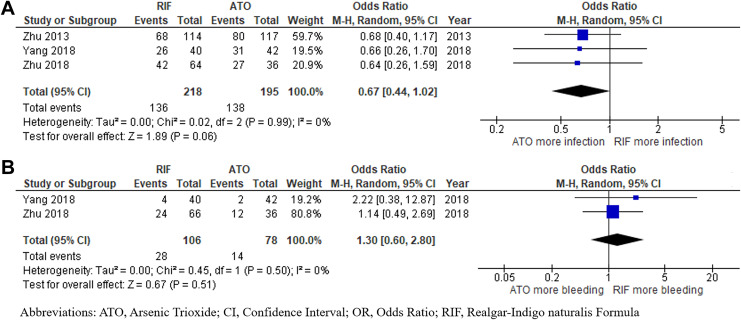
Acute promyelocytic leukemia, a subtype of acute myeloid leukemia, is highly curable. In subgroup of patients with non-high-risk acute promyelocytic leukemia, intravenous arsenic trioxide plus all-trans-retinoic acid is considered the preferred regimen for acute promyelocytic leukemia. Recently, there are interests in the use of the oral form of arsenic, named the Realgar-Indigo naturalis formula, but the data on its efficacy and safety are still relatively limited. The current study was conducted with the aims to identify and summarize the results of all available randomized-controlled studies. A systematic review was conducted in the 2 major databases, utilizing the terms for arsenic and acute promyelocytic leukemia. Eligible studies had to be randomized-controlled studies that compared efficacy and/or adverse effects of oral arsenic versus intravenous arsenic for treatment of patients with acute promyelocytic leukemia. The Mantel-Haenszel method was used to pool the effect estimates and 95% confidence intervals of the included studies together. A total of 4 randomized controlled studies with 482 patients with acute promyelocytic leukemia (258 in Realgar-Indigo naturalis formula group and 224 in intravenous arsenic trioxide group) were included in the meta-analysis. The chances of achieving complete remission were numerically higher in the Realgar-Indigo naturalis formula group but the difference was not statistically significant (pooled odds ratio: 4.59, 95% CI: 0.74-28.57, I2 = 0%). Similarly, other efficacy outcomes, including 30-day mortality rate, overall survival, and event-free survival, also tended to favor the Realgar-Indigo naturalis formula group but the difference was not statistically significant. There was no significant difference in the chance of developing differentiation syndrome, cardiac complications, grades 3 to 4 liver toxicity, grades 3 to 4 renal toxicity, and infection between the 2 groups. The results may suggest that all-trans-retinoic acid plus oral Realgar-Indigo naturalis formula regimen is, at minimum, not a worse alternative to the standard all-trans-retinoic acid plus intravenous intravenous arsenic trioxide regimen for treatment of acute promyelocytic leukemia, especially for patients with low-to-intermediate risk.
Keywords: APL; acute promyelocytic leukemia; arsenic Realgar-Indigo naturalis formula; arsenic trioxide.
Conflict of interest statement
Figures





References
-
- Tallman MS, Altman JK. How I treat acute promyelocytic leukemia. Blood. 2009;114(25):5126-5135. - PubMed
-
- Sanz MA, Lo Coco F, Martín G, et al. Definition of relapse risk and role of nonanthracycline drugs for consolidation in patients with acute promyelocytic leukemia: a joint study of the PETHEMA and GIMEMA cooperative groups. Blood. 2000;96(4):1247–1253. - PubMed
-
- Platzbecker U, Avvisati G, Cicconi L, et al. Improved outcomes with retinoic acid and arsenic trioxide compared with retinoic acid and chemotherapy in non-high-risk acute promyelocytic leukemia: final results of the randomized Italian-German APL0406 trial. J Clin Oncol. 2017;35(6):605–612. - PubMed
-
- Lo-Coco F, Avvisati G, Vignetti M, et al. Retinoic acid and arsenic trioxide for acute promyelocytic leukemia. N Engl J Med. 2013;369(2):111–121. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
