

Anti-migraine Calcitonin Gene-Related Peptide Receptor Antagonists Worsen Cerebral Ischemic Outcome in Mice
- PMID: 32583883
- PMCID: PMC7540520
- DOI: 10.1002/ana.25831
Anti-migraine Calcitonin Gene-Related Peptide Receptor Antagonists Worsen Cerebral Ischemic Outcome in Mice
Abstract
Objective: Calcitonin gene-related peptide (CGRP) pathway inhibitors are emerging treatments for migraine. CGRP-mediated vasodilation is, however, a critical rescue mechanism in ischemia. We, therefore, investigated whether gepants, small molecule CGRP receptor antagonists, worsen cerebral ischemia.
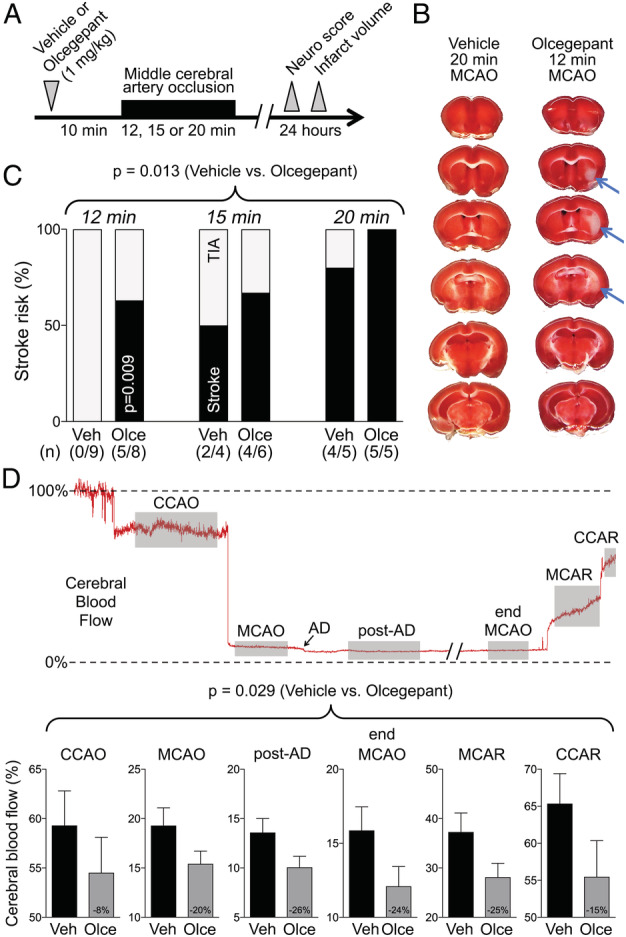
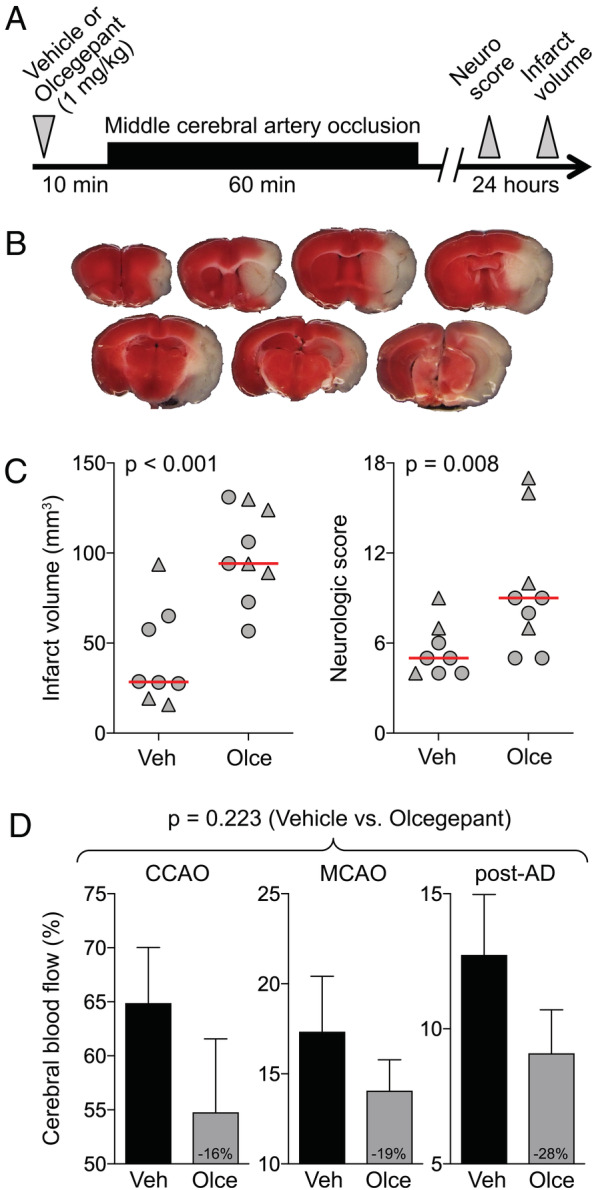
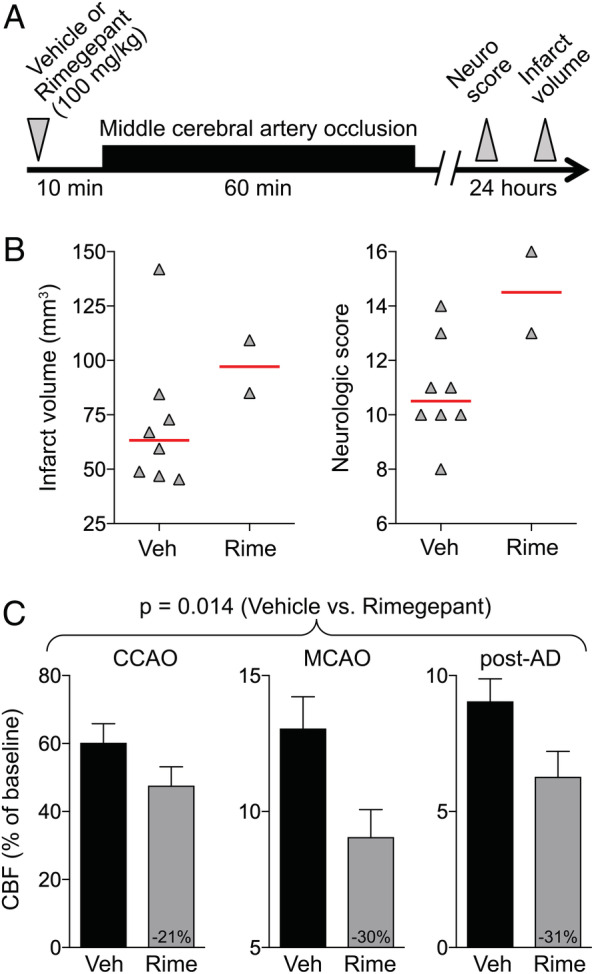
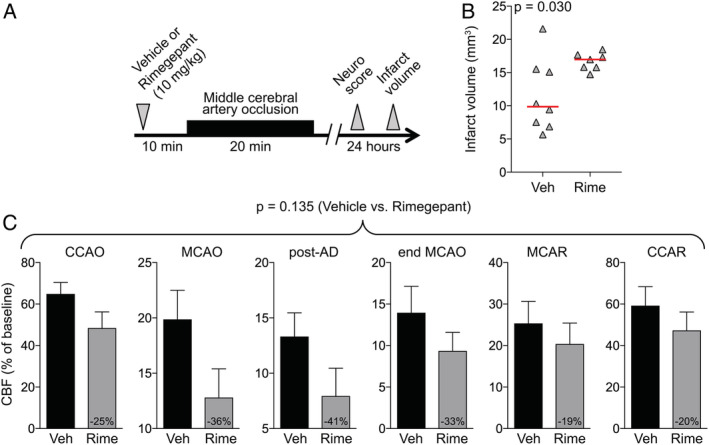
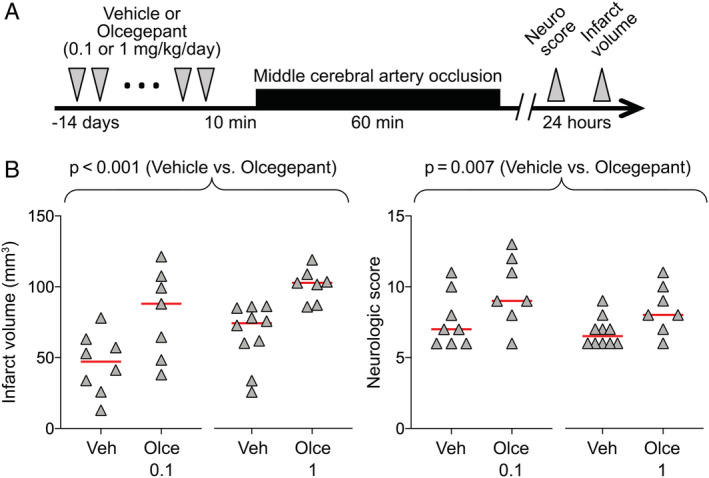
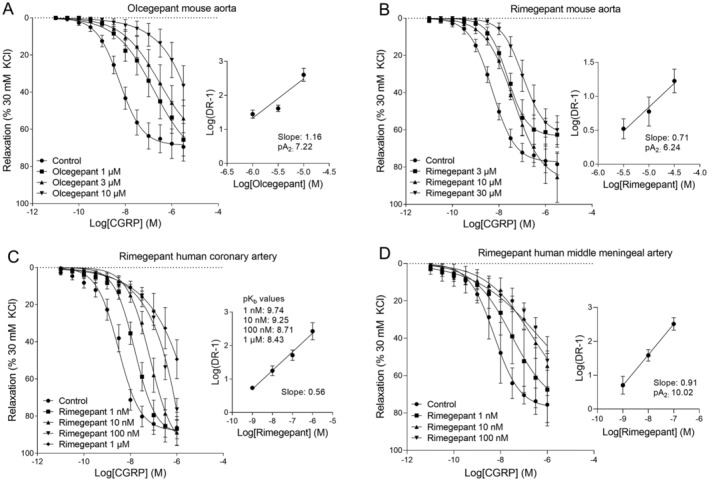
Methods: Middle cerebral artery was occluded for 12 to 60 minutes in mice. We compared infarct risk and volumes, collateral flow, and neurological deficits after pretreatment with olcegepant (single or 10 daily doses of 0.1-1mg/kg) or rimegepant (single doses of 10-100mg/kg) versus vehicle. We also determined their potency on CGRP-induced relaxations in mouse and human vessels, in vitro.
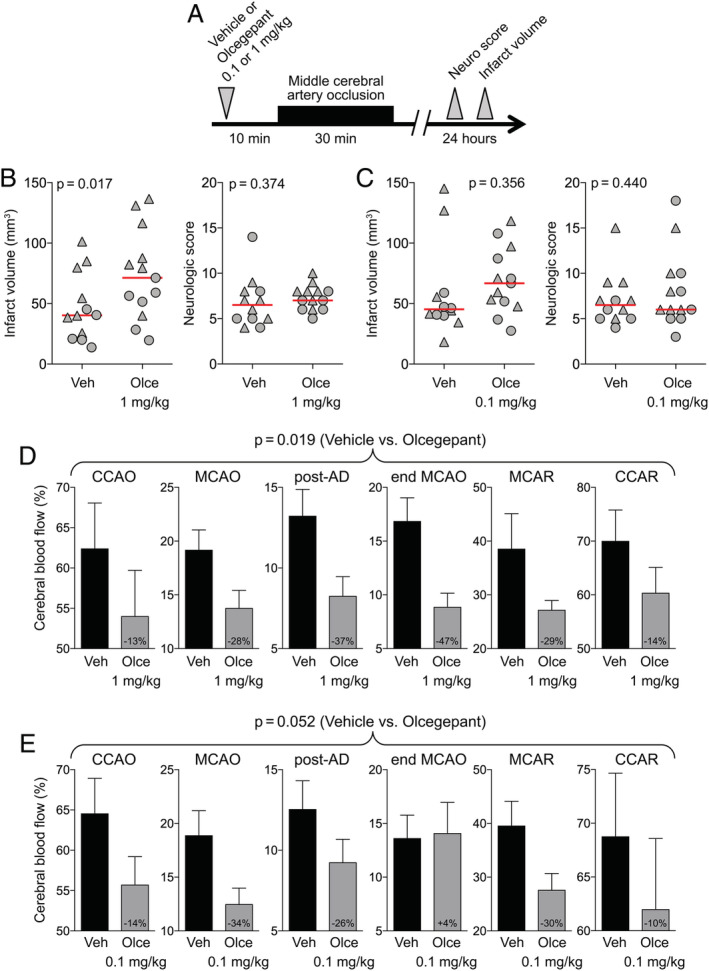
Results: Olcegepant (1mg/kg, single dose) increased infarct risk after 12- to 20-minute occlusions mimicking transient ischemic attacks (14/19 vs 6/18 with vehicle, relative risk = 2.21, p < 0.022), and doubled infarct volumes (p < 0.001) and worsened neurological deficits (median score = 9 vs 5 with vehicle, p = 0.008) after 60-minute occlusion. Ten daily doses of 0.1 to 1mg/kg olcegepant yielded similar results. Rimegepant 10mg/kg increased infarct volumes by 60% after 20-minute ischemia (p = 0.03); 100mg/kg caused 75% mortality after 60-minute occlusion. In familial hemiplegic migraine type 1 mice, olcegepant 1mg/kg increased infarct size after 30-minute occlusion (1.6-fold, p = 0.017). Both gepants consistently diminished collateral flow and reduced reperfusion success. Olcegepant was 10-fold more potent than rimegepant on CGRP-induced relaxations in mouse aorta.
Interpretation: Gepants worsened ischemic stroke in mice via collateral dysfunction. CGRP pathway blockers might thus aggravate coincidental cerebral ischemic events. The cerebrovascular safety of these agents must therefore be better delineated, especially in patients at increased risk of ischemic events or on prophylactic CGRP inhibition. ANN NEUROL 2020;88:771-784.
© 2020 The Authors. Annals of Neurology published by Wiley Periodicals LLC on behalf of American Neurological Association.
Conflict of interest statement
A.M. has received research grants and/or consultant fees from Amgen/Novartis, Lilly, and Teva, which develop anti‐CGRP and/or antimigraine therapeutics. C.A. has received research grants from electroCore, which develops an antimigraine neuromodulation device. M.D.F. receives consultant fees from Company Medtronic, Novartis, Lilly, and Teva, which develop anti‐CGRP and/or antimigraine therapeutics. All companies listed above may be affected by the study.
Figures
References
-
- Edvinsson L, Haanes KA, Warfvinge K, Krause DN. CGRP as the target of new migraine therapies—successful translation from bench to clinic. Nat Rev Neurol 2018;14:338–350. - PubMed
-
- Sparrow AM, Searles JW. The market for migraine drugs. Nat Rev (2019). - PubMed
-
- Hong KW, Pyo KM, Lee WS, et al. Pharmacological evidence that calcitonin gene‐related peptide is implicated in cerebral autoregulation. Am J Physiol 1994;266(pt 2:H11–H16. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
