

Association Between Spine Surgery and Availability of Opioid Medication
- PMID: 32584410
- PMCID: PMC7317600
- DOI: 10.1001/jamanetworkopen.2020.8974
Association Between Spine Surgery and Availability of Opioid Medication
Abstract
Importance: Prolonged prescribing of opioids after spine surgery is often perceived as a negative outcome, but successful opioid reduction may occur despite continued prescribing. Improved characterization of opioid availability before and after surgery is necessary to identify these successes.
Objective: To evaluate the association between spine surgery and modification of opioid availability postoperatively by using consistent definitions to classify opioid availability before and after surgery.
Design, setting, and participants: This population-based cohort study included 2223 adults (age ≥18 years) who underwent spine surgery in Olmsted County, Minnesota, from January 1, 2005, through December 31, 2016. Data were analyzed from April 1, 2019, to December 1, 2019.
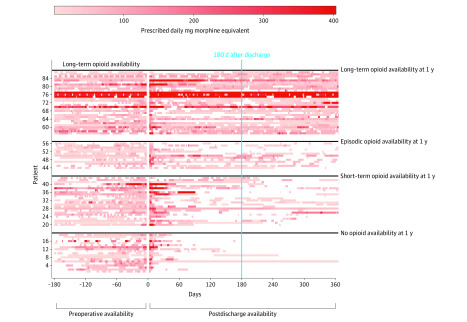
Exposures: Preoperative opioid availability based on prescription data in the 180 days before surgery in accordance with Consortium to Study Opioid Risks and Trends (CONSORT) definitions.
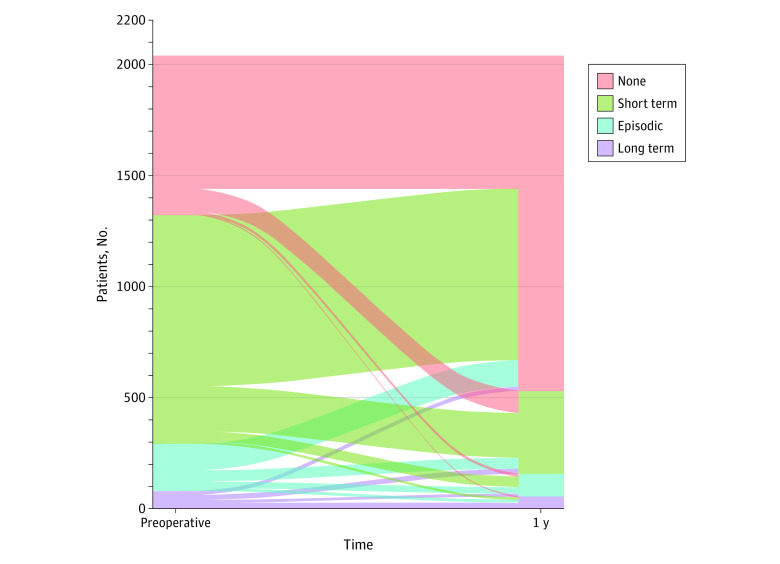
Main outcomes and measures: Successful modification of opioid availability, defined as an improvement in CONSORT status postoperatively (assessed from 181 to 365 days after surgery) compared with preoperative status, or continued absence of opioid availability for patients with no preoperative availability. Multivariable logistic regression was used to assess the association between preoperative opioid availability and successful modification by 1 year after undergoing surgery.
Results: Of 2223 patients included in the study, 1214 were male (54.6%), with a median age of 55 years (interquartile range, 43-68) years. Patients were classified as having no (778 [35.0%]), short-term (1118 [50.3%]), episodic (227 [10.2%]), or long-term (100 [4.5%]) preoperative opioid availability. Of the 2148 patients (96.6%) who were alive at 1 year, postoperative opioid availability was classified as no (1583 [73.7%]), short-term (398 [18.5%]), episodic (104 [4.8%]), and long-term (63 [2.9%]). A total of 1672 patients (77.8%) had successful modification of opioid availability, with success of 83.0% for those with no preoperative availability, 74.9% for those with short-term preoperative availability, 79.8% for those with episodic preoperative availability, and 64.4% for those with long-term preoperative opioid availability. In multivariable analysis, success was significantly associated with preoperative opioid availability (odds ratio [OR] for short term, 0.61 [95% CI, 0.48-0.77]; OR for episodic, 0.95 [95% CI, 0.64-1.40]; OR long term, 0.49 [95% CI, 0.30-0.82]; P < .001 overall vs no availability).
Conclusions and relevance: In this study, when following standardized CONSORT definitions, 4 of 5 adults undergoing spine surgery in a population-based cohort met the criteria for a successful pattern of postoperative opioid prescribing. Similar methods to objectively assess changes in opioid prescribing may be clinically useful in other perioperative settings.
Conflict of interest statement
Figures
Comment in
-
Redefining Opioid Use Patterns After Surgical Procedures: Why a New Paradigm Is Critical.JAMA Netw Open. 2020 Jun 1;3(6):e209457. doi: 10.1001/jamanetworkopen.2020.9457. JAMA Netw Open. 2020. PMID: 32584405 No abstract available.
Similar articles
-
Association Between Preoperative Opioid and Benzodiazepine Prescription Patterns and Mortality After Noncardiac Surgery.JAMA Surg. 2019 Aug 1;154(8):e191652. doi: 10.1001/jamasurg.2019.1652. Epub 2019 Aug 21. JAMA Surg. 2019. PMID: 31215988 Free PMC article.
-
Associations between preoperative opioids, posthospitalization discharge disposition, and long-term opioid prescribing after spine surgery: a population-based cohort study.Asian Spine J. 2025 May 30. doi: 10.31616/asj.2024.0414. Online ahead of print. Asian Spine J. 2025. PMID: 40451618
-
Association Between Preoperative Benzodiazepine Use and Postoperative Opioid Use and Health Care Costs.JAMA Netw Open. 2020 Oct 1;3(10):e2018761. doi: 10.1001/jamanetworkopen.2020.18761. JAMA Netw Open. 2020. PMID: 33107919 Free PMC article.
-
Long-Term Opioid Prescriptions After Spine Surgery: A Meta-Analysis of Prevalence and Risk Factors.World Neurosurg. 2020 Sep;141:e894-e920. doi: 10.1016/j.wneu.2020.06.081. Epub 2020 Jun 19. World Neurosurg. 2020. PMID: 32569762
-
Congress of Neurological Surgeons Systematic Review and Evidence-Based Guidelines for Perioperative Spine: Preoperative Opioid Evaluation.Neurosurgery. 2021 Oct 13;89(Suppl 1):S1-S8. doi: 10.1093/neuros/nyab315. Neurosurgery. 2021. PMID: 34490881
Cited by
-
The potential for diversion of prescribed opioids among orthopaedic patients: Results of an anonymous patient survey.PLoS One. 2021 Aug 26;16(8):e0256741. doi: 10.1371/journal.pone.0256741. eCollection 2021. PLoS One. 2021. PMID: 34437639 Free PMC article.
-
An Update on Postoperative Opioid Use and Alternative Pain Control Following Spine Surgery.Orthop Rev (Pavia). 2021 Jun 22;13(2):24978. doi: 10.52965/001c.24978. eCollection 2021. Orthop Rev (Pavia). 2021. PMID: 34745473 Free PMC article. Review.
-
Patterns and Outcomes of Opioid Use Before and After Hospitalization for Critical Illness: A Population-Based Cohort Study.J Intensive Care Med. 2025 Jan;40(1):85-93. doi: 10.1177/08850666241268473. Epub 2024 Aug 6. J Intensive Care Med. 2025. PMID: 39105427
-
Prescription Opioids and Brain Structure in Community-Dwelling Older Adults.Mayo Clin Proc. 2024 May;99(5):716-726. doi: 10.1016/j.mayocp.2024.01.018. Mayo Clin Proc. 2024. PMID: 38702125 Free PMC article.
-
Different Gabapentin and Pregabalin Dosages for Perioperative Pain Control in Patients Undergoing Spine Surgery: A Systematic Review and Network Meta-Analysis.JAMA Netw Open. 2023 Aug 1;6(8):e2328121. doi: 10.1001/jamanetworkopen.2023.28121. JAMA Netw Open. 2023. PMID: 37556139 Free PMC article.
References
-
- Jain N, Phillips FM, Weaver T, Khan SN. Preoperative chronic opioid therapy: a risk factor for complications, readmission, continued opioid use and increased costs after one- and two-level posterior lumbar fusion. Spine (Phila Pa 1976). 2018;43(19):1331-1338. doi:10.1097/BRS.0000000000002609 - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
