

Outcomes of incident atrial fibrillation in heart failure with preserved or reduced ejection fraction: A community-based study
- PMID: 32584498
- PMCID: PMC8562322
- DOI: 10.1111/jce.14632
Outcomes of incident atrial fibrillation in heart failure with preserved or reduced ejection fraction: A community-based study
Abstract
Introduction: The best management strategy for patients with atrial fibrillation (AF) with heart failure (HF) and preserved left ventricular ejection fraction (LVEF) is unknown.
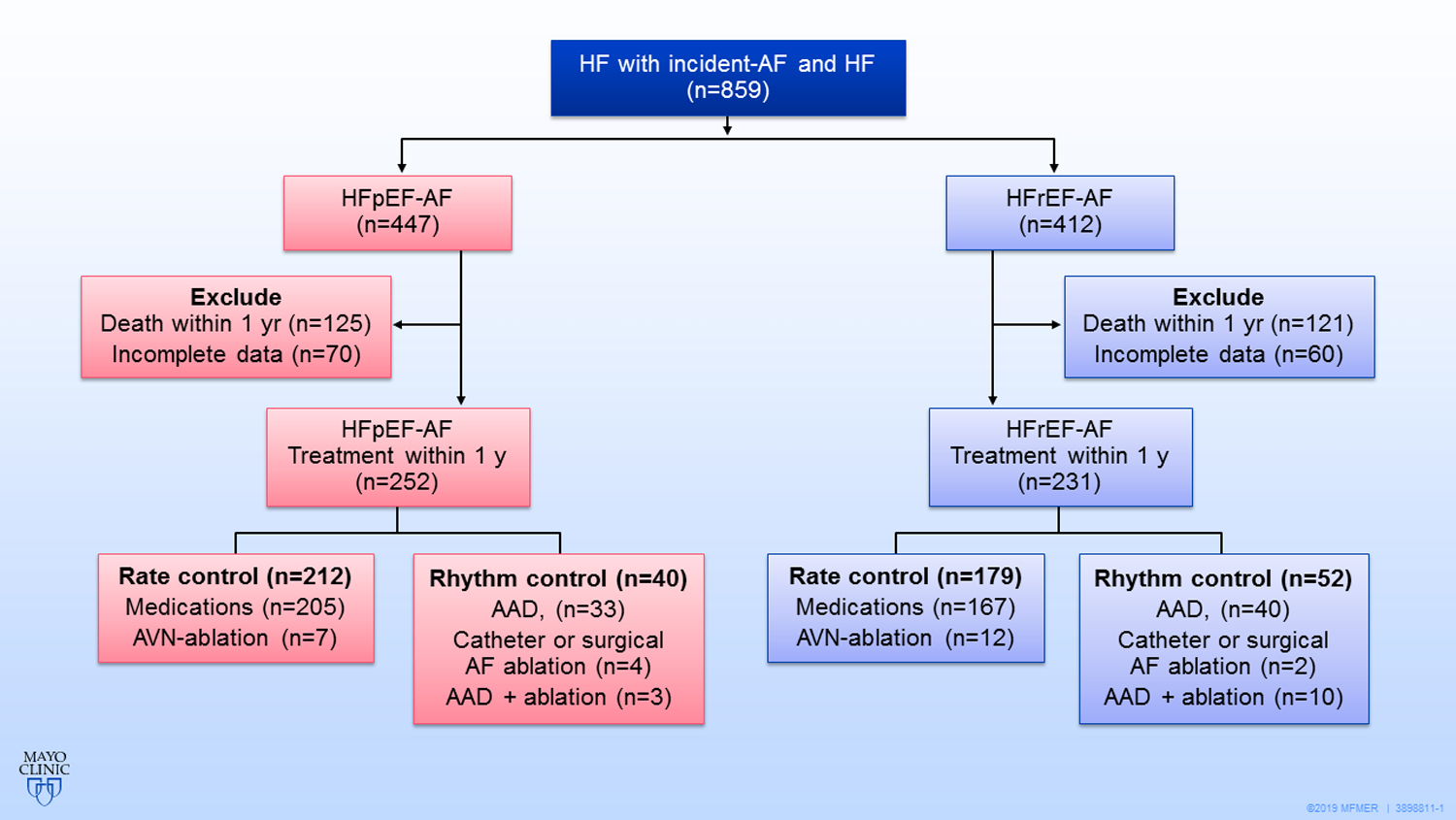
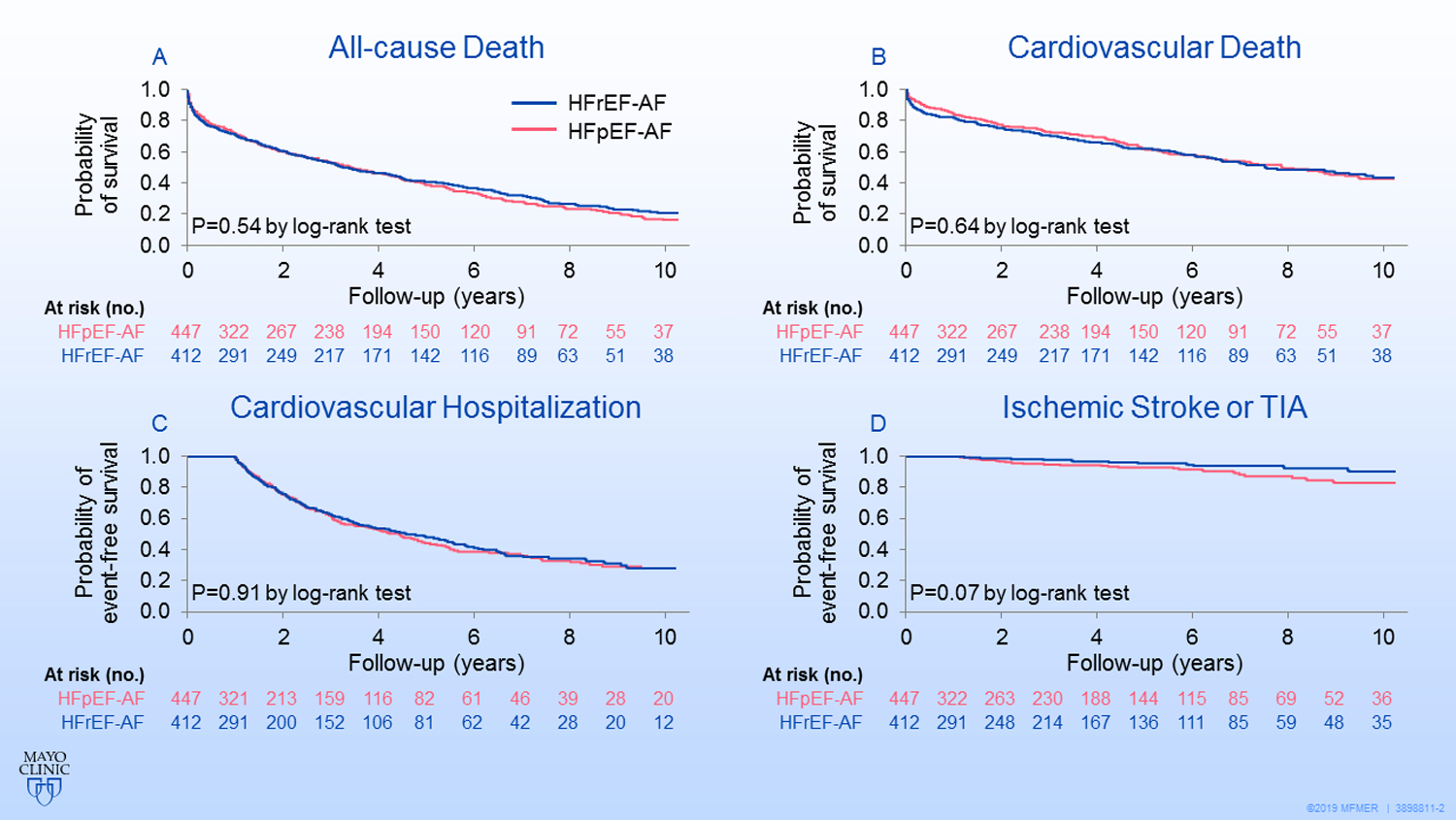
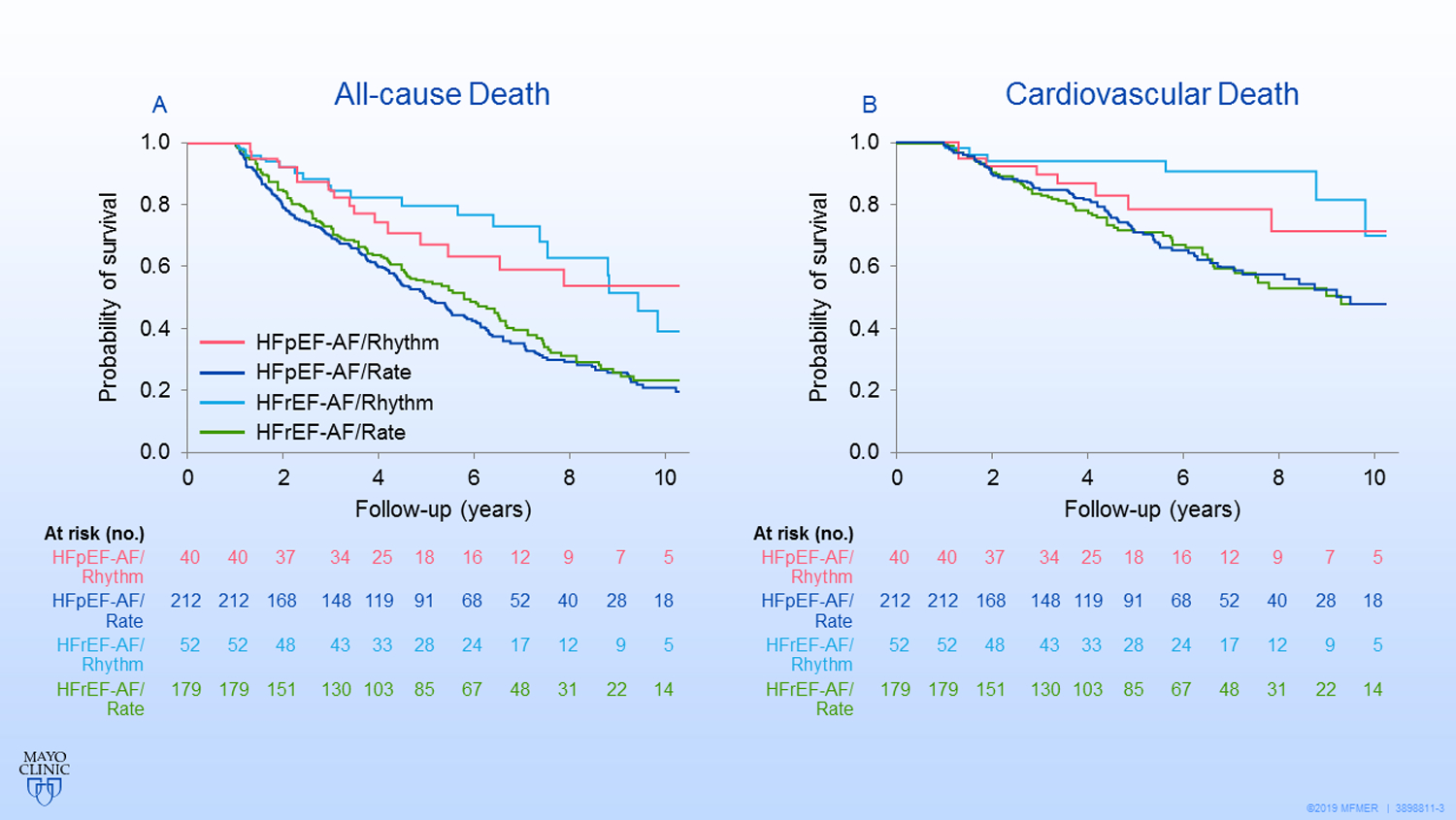
Methods and results: This cohort study was conducted in Olmsted County, Minnesota, with resources of the Rochester Epidemiology Project. Patients with incident AF occurring between 2000 and 2014 with a prior or concurrent HF were included. Patients with LVEF ≥ 50% were designated as HF and preserved ejection fraction (HFpEF) and those with LVEF < 50% were designated as HF and reduced ejection fraction (HFrEF). Rhythm control in the first year after AF diagnosis was defined as prescriptions for an antiarrhythmic drug, catheter ablation, or maze procedure. The primary endpoint was all-cause mortality. The secondary endpoints were cardiovascular death, cardiovascular hospitalization, and stroke or transient ischemic attack. Of 859 patients (age, 77.2 ± 12.1 years; 49.2%, female), 447 had HFpEF-AF, and 412 had HFrEF-AF. There was no difference in all-cause mortality (10-year mortality, 83% vs 79%; p = .54) or secondary endpoints between the HFpEF-AF and HFrEF-AF, respectively. Compared with the rate control strategy, rhythm control in HFpEF-AF patients (n = 40, 15.9%) offered no survival benefits (adjusted HR, 0.70; 95% CI, 0.42-1.16; p = .16), whereas rhythm control in HFrEF-AF patients (n = 52, 22.5%) decrease cardiovascular mortality (HR, 0.38; 95% CI, 0.17-0.86; p = .02).
Conclusions: Patients with HFpEF-AF and HFrEF-AF had similar poor prognoses. Rhythm control strategy was seldom adopted in community care in patients with HF and AF. A rhythm control strategy may provide survival benefit for patients with HFrEF-AF and the benefit of rhythm control in patients with HFpEF-AF warrants further study.
Keywords: atrial fibrillation; heart failure with preserved ejection fraction; heart failure with reduced ejection fraction; rate control; rhythm control.
© 2020 Wiley Periodicals LLC.
Conflict of interest statement
Conflicts of interest: None
Figures
Similar articles
-
Heart failure progression and mortality in atrial fibrillation patients with preserved or reduced left ventricular ejection fraction.J Interv Card Electrophysiol. 2019 Sep;55(3):325-331. doi: 10.1007/s10840-019-00534-x. Epub 2019 Mar 18. J Interv Card Electrophysiol. 2019. PMID: 30887281
-
Atrial resynchronization therapy in patients with atrial fibrillation and heart failure with and without systolic left ventricular dysfunction: a pilot study.J Interv Card Electrophysiol. 2018 Oct;53(1):9-17. doi: 10.1007/s10840-018-0408-1. Epub 2018 Jul 9. J Interv Card Electrophysiol. 2018. PMID: 29987682
-
Atrial fibrillation and risk of adverse outcomes in heart failure with reduced, mildly reduced, and preserved ejection fraction: A systematic review and meta-analysis.J Cardiovasc Electrophysiol. 2024 Apr;35(4):715-726. doi: 10.1111/jce.16209. Epub 2024 Feb 13. J Cardiovasc Electrophysiol. 2024. PMID: 38348517
-
Atrial fibrillation and risk of incident heart failure with reduced versus preserved ejection fraction.Heart. 2022 Mar;108(5):353-359. doi: 10.1136/heartjnl-2021-319122. Epub 2021 May 24. Heart. 2022. PMID: 34031160 Free PMC article.
-
Atrial Fibrillation Ablation in Heart Failure With Reduced vs Preserved Ejection Fraction: A Systematic Review and Meta-Analysis.JAMA Cardiol. 2024 Jun 1;9(6):545-555. doi: 10.1001/jamacardio.2024.0675. JAMA Cardiol. 2024. PMID: 38656292 Free PMC article.
Cited by
-
Atrial fibrillation is associated with cardiovascular events in obese Japanese with one or more cardiovascular risk factors: The Japan Morning Surge Home Blood Pressure (J-HOP) Study.J Clin Hypertens (Greenwich). 2021 Mar;23(3):665-671. doi: 10.1111/jch.14170. Epub 2021 Jan 6. J Clin Hypertens (Greenwich). 2021. PMID: 33405296 Free PMC article.
-
Safety, Efficacy and Prognostic Benefit of Atrial Fibrillation Ablation in Heart Failure with Preserved Ejection Fraction.Arrhythm Electrophysiol Rev. 2022 Apr;11:e18. doi: 10.15420/aer.2022.10. Arrhythm Electrophysiol Rev. 2022. PMID: 36304203 Free PMC article. Review.
-
Rhythm versus rate control for atrial fibrillation in heart failure with preserved ejection fraction.Heart Rhythm O2. 2022 Jun 30;3(5):520-525. doi: 10.1016/j.hroo.2022.06.009. eCollection 2022 Oct. Heart Rhythm O2. 2022. PMID: 36340484 Free PMC article.
-
Embarking upon atrial fibrillation management in heart failure with preserved ejection fraction: Charting a course.J Cardiovasc Electrophysiol. 2020 Sep;31(9):2284-2287. doi: 10.1111/jce.14635. Epub 2020 Jul 1. J Cardiovasc Electrophysiol. 2020. PMID: 32583508 Free PMC article. No abstract available.
-
Atrial fibrillation ablation in heart failure with mid-range ejection fraction: Is it time to open the champagne?Indian Pacing Electrophysiol J. 2023 Sep-Oct;23(5):142-143. doi: 10.1016/j.ipej.2023.08.004. Indian Pacing Electrophysiol J. 2023. PMID: 37652619 Free PMC article. No abstract available.
References
-
- Benjamin EJ, Muntner P, Alonso A, et al. Heart Disease and Stroke Statistics-2019 Update: A Report From the American Heart Association. Circulation. 2019;139(10):e56–e528. - PubMed
-
- Wang TJ, Massaro JM, Levy D, et al. A risk score for predicting stroke or death in individuals with new-onset atrial fibrillation in the community: the Framingham Heart Study. JAMA. 2003;290(8):1049–1056. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
