

Serial Measurement of Cell-Cycle Arrest Biomarkers [TIMP-2] · [IGFBP7] and Risk for Progression to Death, Dialysis, or Severe Acute Kidney Injury in Patients with Septic Shock
- PMID: 32584598
- PMCID: PMC7605192
- DOI: 10.1164/rccm.201906-1197OC
Serial Measurement of Cell-Cycle Arrest Biomarkers [TIMP-2] · [IGFBP7] and Risk for Progression to Death, Dialysis, or Severe Acute Kidney Injury in Patients with Septic Shock
Abstract
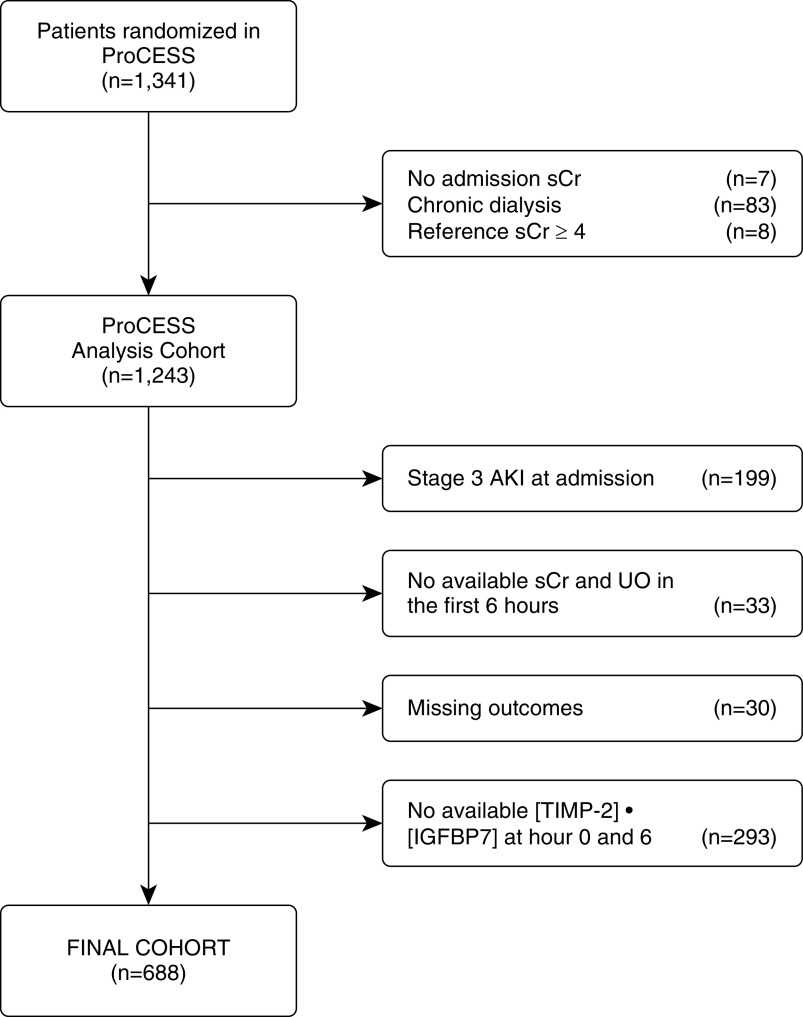
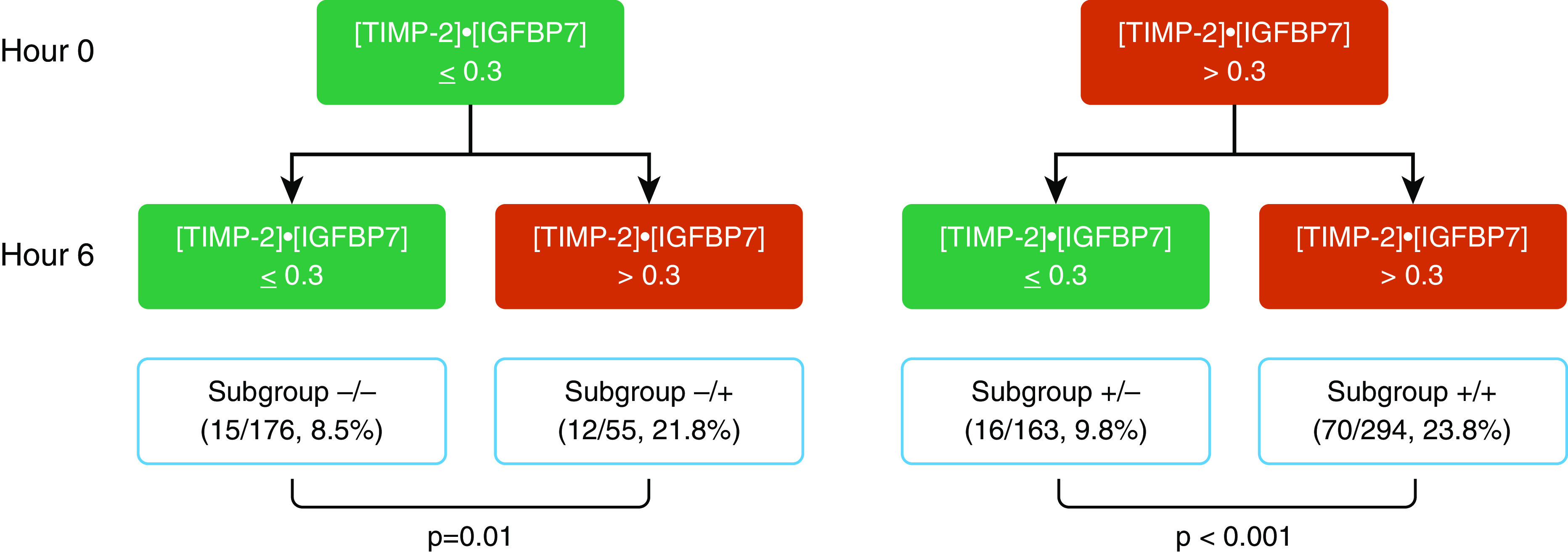
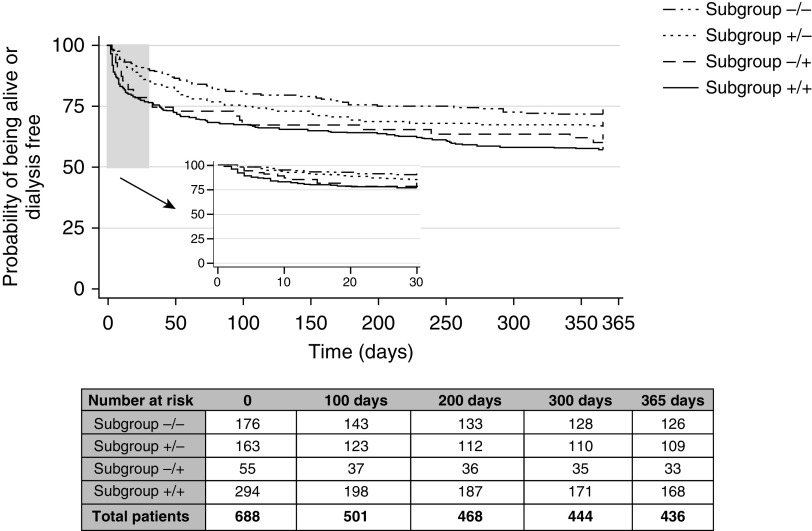
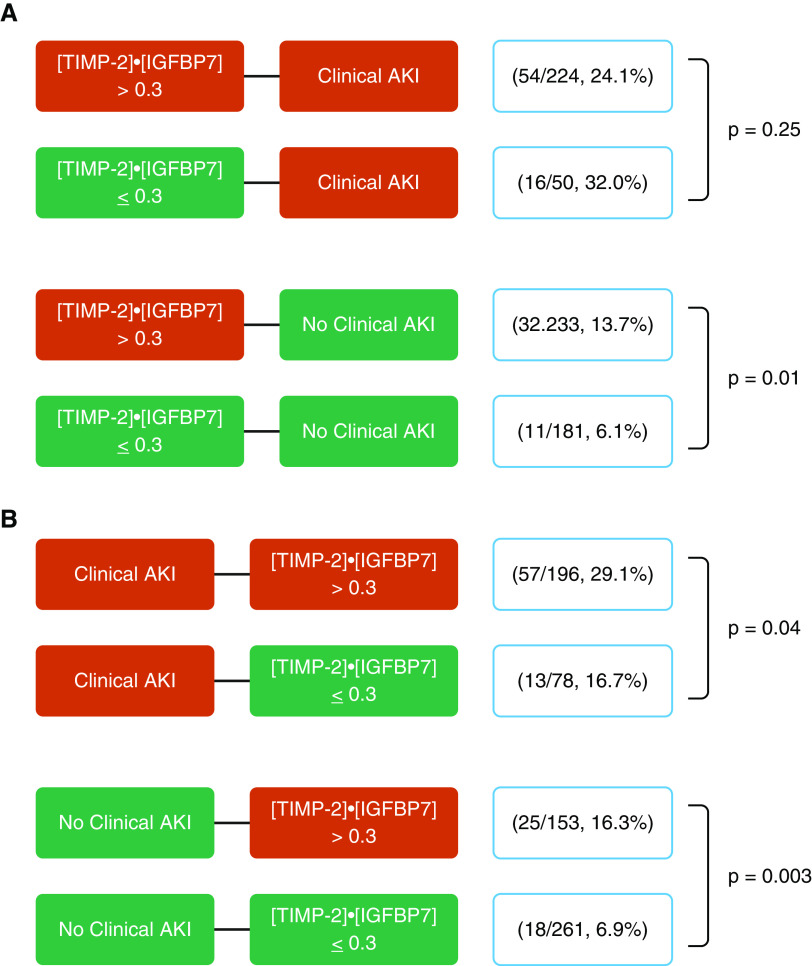
Rationale: Urinary TIMP-2 (tissue inhibitor of metalloproteinases-2) and IGFBP7 (insulin-like growth factor-binding protein 7) can predict acute kidney injury (AKI) in patients with sepsis.Objectives: To address critical questions about whether biomarkers can inform the response to treatment and whether they might be used to guide therapy, as most sepsis patients present with AKI.Methods: We measured [TIMP-2] · [IGFBP7] before and after a 6-hour resuscitation in 688 patients with septic shock enrolled in the ProCESS (Protocol-based Care for Early Septic Shock) trial. Our primary endpoint was stage 3 AKI, renal replacement therapy, or death within 7 days.Measurements and Main Results: The endpoint was reached in 113 patients (16.4%). In patients with negative [TIMP-2] · [IGFBP7] at baseline, those who became positive (>0.3 U) after resuscitation had three-times higher risk compared with those who remained negative (21.8% vs. 8.5%; P = 0.01; odds ratio [OR], 3.0; 95% confidence interval [CI], 1.31-6.87). Conversely, compared with patients with a positive biomarker at baseline that were still positive at Hour 6, risk was reduced for patients who became negative (23.8% vs. 9.8%; P = 0.01; OR, 2.15; 95% CI, 1.17-3.95). A positive [TIMP-2] · [IGFBP7] after resuscitation was associated with worse outcomes in both patients with and without AKI at that time point. The clinical response to resuscitation, as judged by the Acute Physiology and Chronic Health Evaluation II score, was weakly predictive of the endpoint (area under the curve, 0.68; 95% CI, 0.62-0.73) and improved with addition of [TIMP-2] · [IGFBP7] (0.72; 95% CI, 0.66-0.77; P = 0.03). Different resuscitation protocols did not alter biomarker trajectories, nor did they alter outcomes in biomarker-positive or biomarker-negative patients. However, biomarker trajectories were associated with outcomes.Conclusions: Changes in urinary [TIMP-2] · [IGFBP7] after initial fluid resuscitation identify patients with sepsis who have differing risk for progression of AKI.Clinical trial registered with www.clinicaltrials.gov (NCT00510835).
Keywords: acute kidney injury; cell-cycle arrest biomarkers; dialysis; sepsis; survival.
Figures
Comment in
-
Trajectory of Kidney Function: The Canary in Sepsis.Am J Respir Crit Care Med. 2020 Nov 1;202(9):1211-1212. doi: 10.1164/rccm.202007-2627ED. Am J Respir Crit Care Med. 2020. PMID: 32716638 Free PMC article. No abstract available.
References
-
- Hoste EA, Bagshaw SM, Bellomo R, Cely CM, Colman R, Cruz DN, et al. Epidemiology of acute kidney injury in critically ill patients: the multinational AKI-EPI study. Intensive Care Med. 2015;41:1411–1423. - PubMed
-
- Kellum JA, Bellomo R, Ronco C. Kidney attack. JAMA. 2012;307:2265–2266. - PubMed
-
- Uchino S, Kellum JA, Bellomo R, Doig GS, Morimatsu H, Morgera S, et al. Beginning and Ending Supportive Therapy for the Kidney (BEST Kidney) Investigators. Acute renal failure in critically ill patients: a multinational, multicenter study. JAMA. 2005;294:813–818. - PubMed
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
